
S. Helmy
National Institute of Urology and Nephrology, Cairo, Egypt
A. El-Shenoufy
Faculty of Medicine, Cairo University, Cairo, Egypt
Journal of Biological Sciences
Year: 2009 | Volume: 9 | Issue: 7 | Page No.: 766-771







ABSTRACT
Evaluation of the effectiveness of a cheaper newly developed web cam trainer to assist surgeons in developing basic laparoscopic skills in comparison to other inexpensive trainers was our objective to make this study. This newly developed web cam trainer consists of a web cam (equipped with a light source and light sensor), a foam box and a home computer. This homemade trainer was compared to the cardboard trainer developed by End urology Institute, Cedars-Sini Medical Center, which consists of a web cam, a cardboard box, a desk lamp and a home computer. A total of twelve participants at the National Institute of Urology and Nephrology, Cairo, Egypt were divided into two groups each using both trainers to perform basic tasks (pattern cutting and suturing the skin of a raw chicken). Time of the participants to perform each task was used to evaluate the effectiveness of both trainers (performance time). Statistical analysis of the 3 tasks comparing between this web cam trainer and the cardboard web trainer, developed by end urology Institute, Cedars-Sini Medical Canter, showed no statistical significance between both web trainers during performing task 1 (p = 0.590), but there was significant statistical difference during performing tasks 2 and 3 (p≤0.001). We conclude that this web cam pelvitrainer simulates for novice laparoscopists an easier way to develop basic laparoscopy skills without the need for expensive instruments and specialized training centers. In addition, the ability to review recorded tasks allows the trainee to learn their mistakes and how to overcome them. It is also superior to the cardboard trainer in performing tasks requiring complex skills.
PDF Abstract XML References Citation
How to cite this article
S. Helmy and A. El-Shenoufy, 2009. Development of Laparoscopic Skills using a New Inexpensive Webcam Trainer. Journal of Biological Sciences, 9: 766-771.
DOI: 10.3923/jbs.2009.766.771
URL: https://scialert.net/abstract/?doi=jbs.2009.766.771
DOI: 10.3923/jbs.2009.766.771
URL: https://scialert.net/abstract/?doi=jbs.2009.766.771
INTRODUCTION
During the last decade, laparoscopy has changed the surgical approach to many surgical procedures. Urologic procedures, in which laparoscopy has become the standard approach, are increasing every day; this entitles that all junior urologists attain basic laparoscopic training (Shalhav et al., 2002).
There is a consensus among surgeons that laparoscopic procedures with low and middle level of difficulty are part of the general surgical training (Fitzgibbons and Puri, 2006).
The data received from several surgical training studies clearly demonstrate that the modular programme enables the young surgeons to develop the requisite skills rapidly to master a complex procedure such as radical prostatectomy (Stolzenburg et al., 2005, 2006).
Earlier studies have demonstrated the importance of laparoscopic training at the residency level and its profound effect on the future practices of graduates (Shay et al., 2002). Despite the increasing performance of laparoscopy from current graduates (Wang and Winfield, 2004), other recent data continue to demonstrate that most graduating residents still do not consider their laparoscopic experience satisfactory (Duchene et al., 2006). The current state of laparoscopic training at the resident level, however, has not been well delineated and we have a poor understanding of the preparedness of the residents to perform this procedure.
Teaching operative skills is of paramount importance to urology resident training. Halstead first introduced a mentor-trainee model that has been applied for long as a scheme for teaching conventional surgical techniques to residents (Barnes et al., 1989).
A vast variety of simulators and models for laparoscopic training in urology and general surgery with different levels of validity and reliability are available (Feldman et al., 2004). The expensive technology involved in laparoscopic training is a factor in delaying the advancement of laparoscopy in many institutions especially in developing countries (Shalhav et al., 2002).
This has been overcome by the introduction and further development of inexpensive, mobile methods used to learn and reinforce laparoscopic skills namely web cam trainers, which have been proven to be as effective as commercially available trainers (Mughal, 1992; Gue, 1995). We report our initial experience with a simple, inexpensive web cam system and set up of materials readily available. We compared its effectiveness to that of other cheap web cam trainers.
MATERIALS AND METHODS
This study was conducted during the months of January and June 2008, at the Urology Department, Faculty of Medicine, Cairo University and the National Institute of Urology and Nephrology, Egypt.
The web cam laparoscopic training device is composed of an inexpensive web cam (2B, China) equipped with a light source, a foam box and a laptop computer (Fig. 1). This was compared to another web cam trainer developed by End Urology Institute, Cedars-Sini Medical Center, which consists of a web cam, a cardboard box, a desk lamp and a home computer (Fig. 2). Disposable, expired laparoscopic instruments were also used (Chung et al., 2005).
A total of twelve participants without prior laparoscopic training were enrolled in the study and asked to execute three basic tasks: shape fitting task 1, patterned cutting task 2 and suturing the skin of a raw chicken leg task 3. Task 1 consisted of attempting to fit block shapes into their places into a stencil (Fig. 3a, b). Task 2 consisted of using endoscopic scissors to trail a pattern drawn on the skin of a raw chicken leg (Fig. 4).
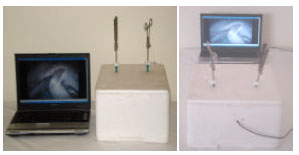 | |
| Fig. 1: | New web cam laparoscopic training device |
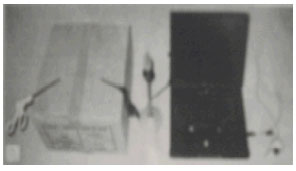 | |
| Fig. 2: | Web cam trainer developed by End urology Institute, Cedars-Sini Medical Center (Chung et al., 2005) |
Task 3 consisted of suturing the skin of a raw chicken leg (Fig. 5). The 12 participants were divided into two groups. Each group performed both tasks on both web cam trainers. Their level of performance was measured by the time needed to complete both tasks. Differences between the two groups were analyzed by the Mann-Whitney test to calculate the p-value, where a p<0.05 was considered statistically significant.
 | |
| Fig. 3: | (a, b): Task 1, basic tasks |
 | |
| Fig. 4: | Task 2, Endoscopic scissors to trail a pattern drawn on the skin of a raw chicken leg |
 | |
| Fig. 5: | Task 4, suturing the skin of a raw chicken leg |
RESULTS AND DISCUSSION
The time to complete each task (performance time) was measured for each of the 12 trainees, once using our newly developed trainer and once using the cardboard pelvitrainer. Numbers were assigned to each candidate and the numbers were randomly selected. The first 6 numbers to be selected should have performed the first task (shape fitting) on our pelvitrainer, followed by the cardboard pelvitrainer and the performance time for each candidate to complete the task. This was followed by measuring performance of the second and third tasks (patterned cutting and suturing raw chicken leg). Trainers should start with our new pelvitrainer, followed by performing same tasks using the cardboard pelvitrainer and the performance time for each candidate to complete the task. The other 6 candidates to be selected performed the same tasks with reverse order of the pelvitrainers used. The performance time for each candidate to complete each task using each pelvitrainer was measured. This is followed by a random selection of the order in which the candidates performed the tasks on each pelvitrainer to eliminate the error that could arise from a candidate repeating the same task for a second time on a different pelvitrainer. Repetition of the same task familiarizes the candidate more with the configuration of the pelvitrainers, equipment used and hand-eye coordination (learning curve).
For task 1 (shape fitting) the mean performance time of the 12 trainees using the cardboard pelvitrainer is (169.5±16.54 sec) which was slightly higher than the mean performance time of (166.2±15.88 sec) using our pelvitrainer. The paired difference being statistically insignificant (p = 0.590). For task 2 (patterned cutting) there was a large difference in performance time using each pelvitrainer; the mean performance time of the 12 trainees using the cardboard pelvitrainer was 773.8±44.89 sec and the mean performance time using our pelvitrainer was 589.5±53.72 sec. The paired difference being statistically significant (p≤0.001). With regard to task 3 (suturing of a raw chicken leg) there was a similar difference using each pelvitrainer as seen in task 2; the mean performance time of the 12 trainees using the cardboard pelvitrainer being 1314.7±47.32 sec and the mean performance time using our pelvitrainer being 1064.3±28.42 sec. The paired difference being statistically significant (p≤0.001). The results are summarized in Fig. 6a-c and Table 1.
In conclusion, our pelvitrainer was statistically superior to the cardboard trainer during performing both task 2 and 3, but similar to the cardboard pelvitrainer during performing task 1. Task 1, being a simple procedure involving fitting shapes into their desired gap in the stencil, no statistical difference between each pelvitrainer was noticed. However, task 2 and 3 showed a noticeable difference in results. This was due to complexity, better handling of equipment, hand-eye coordination and precision between the uses of different pelvitrainers. The reason of this success may be attributed to the advantages of our pelvitrainer such as better image transfer, superior illumination and easier handling of laparoscopic instruments through trocar ports.
The era of laparoscopy has created new training needs and demands that are certainly not fulfilled by the existing training modalities. Laparoscopic skills differ to those of open surgery, being more related to endoscopy than to traditional laparotomy. Procedures are performed with the aid of a two dimensional video image, with decreased tactile feedback, paradoxical instrument movements and a limited range of motion (Dagash et al., 2003; Ahlberg et al., 2005; Buchmann and Dincler, 2005; Tang et al., 2005).
| Table 1: | Calculated by Mann-Whitney test |
 | |
 | |
| Fig. 6: | (a-c) Box and whisker graph. The dark horizontal line, the box and the whisker represent the median, the inter-quartile range and the total range, respectively |
Their residencies is indeed a difficult task. Transfer of skills based on techniques learned performing open surgery is neither appropriate nor effective (Colegrove et al., 1999).
The introduction of Laparoscopic trainers have changed the realm of laparoscopic training, allowing the transition from conducting actual surgeries in the operating room to developing basic surgical skills at both dry and wet labs (Hamdorf and Hall, 2000; MacNatt and Smith, 2001; Madan et al., 2003).
Physical simulators include a box trainer and real instruments (as used in the laparoscopic room). The materials used in these simulators can provide texture and behavior similar to real tissues. The measurement method can be scored by a trained observer or by motion-tracking systems. The Southwestern center for minimally invasive surgery tasks, the Rosser tasks and the McGill Inanimate System for Training and Evaluation of Laparoscopic Skills (MISTELS) are the most common simulators of this category (Rosser et al., 1998; Keyser et al., 2000; Risucci et al., 2001; Scott et al., 2001).
The high cost, ranging between 300 and $2500 has limited the availability of such trainers to all urologists. In addition to other limitations such as requiring the urologist presence at trained minimally invasive centers, time and scheduling constraints and the need of expensive accessory equipments like video monitors and endoscopic cameras.
These expensive trainers can be easily and readily duplicated using web cam trainers, providing a cheap, mobile and effective means to teach and develop basic laparoscopic skills. These web cam trainers consist of a web cam, a box, an external light source and a home computer.
Our newly proposed web cam trainer consists of a web cam with a light source, a foam box (used originally to store frozen food) and a laptop computer. The web cam used (U2B, China) has the following features: UBS port 2.0, 1.3 M pixels resolution, large window capture with size 640x480, built-in image compression, light source with an automatic brightness adjuste and a manual adjustment hinge. The cost of this web cam is approximately 9 US dollars.
Having a web cam, with built-in light source, helps in providing a superior and focused lighting of the foam box interior, especially at the working area. This is considered an added feature in our proposed module since using an ordinary external light source will provide less focused lighting at the working area.
Moreover, the automatic light adjuster is responsible for automatically adjusting the power of the light source, keeping a constant stable lighting at the working area. This was found to enhance the trainee’s performance.
The high transmission speed (2.0 UBS) and high resolution (1.3 M pixels) features on our proposed web cam, provides a real-time image during the training sessions, with no delays during image transfer when compared with other traditional web cams. This replaces the need for using the endoscopic camera and video monitor during training.
The idea of using a white foam box is to reflect and provide superior lighting for the box interior. In addition to the ease of puncturing the foam surface using disposable 10 and 5 mm trocar ports. Exact accommodation of the trocar size limits light leakage and stabilizes the trocar in place, in addition to providing a range of mobility similar to the human abdominal wall.
The time to perform task 1 did not differ much from our pelvitrainer with a mean performance time of 166.2 sec and the cardboard trainer the mean performance time of 169.5 sec. We attributed this to the simplicity of the procedure that require only fitting shapes.
On the contrary, the time to perform task 2 (patterned cutting of the chicken skin) showed a significant difference between our pelvitrainer with a mean performance time of 589.5 sec and the cardboard trainer with a mean performance time of 773.8 sec and this may be due to more need for better vision, better instrument handling and better hand-eye coordination.
Similarly, the time to perform task 3 was much less during the use of our pelvitrainer with a mean performance time of 1064.3 sec compared to the mean performance time during the use of cardboard trainer (1314.7 sec). This suturing task also needs more skill, better vision, better instrument handling and better hand-eye coordination and is considered one of the most difficult tasks during laparoscopy training.
The recording capability of the computer used can help trainees preview prior assessments before undergoing laparoscopic operations; moreover, reviewing previous training sessions help trainee to undergo self assessment and upgrade of their skills. This can all be done by just a click of a mouse.
CONCLUSION
We describe our newly developed pelvitrainer as an opportunity for novice laparoscopist to engage in basic laparoscopic training in an environment similar to the ones provided by professional trainers, without the need for expensive equipment and costly sophisticated training facilities. This is not to say that our system may replace essential courses or animal models. However, it may provide a cheap, affordable conduit to enhance training before engaging in standardized protocols of training through which the trainee may practice for timeless hours at their own convenience. Furthermore, the ability of playback sessions may allow for self-assessment and practice via the internet under the supervision of a professional trainer. Comparing our pelvitrainer to the one developed by the End urology Institute, Cedars-Sini Medical Canter proves to be more efficient.
REFERENCES
- Ahlberg, G, O. Kruuna, C.E. Leijonmarck, J. Ovaska and A. Rosseland et al., 2005. Is the learning curve for laparoscopic fundoplication determined by the teacher or the pupil? Am. J. Surg., 189: 184-189.
PubMed - Barnes, R.W., N.P. Lang and M.F. Whiteside, 1989. Halstedian technique revisited: Innovations in teaching surgical skills. Ann. Surg., 210: 118-121.
PubMed - Buchmann, P. and S. Dincler, 2005. Learning curve-calculation and value in laparoscopic surgery. Ther. Umsch., 62: 69-75.
PubMed - Chung, S.Y., D. Landsittel, C.H. Chon, C.S. Ng and G.J. Fuchs, 2005. laparoscopic skills training using a webcam trainer. J. Urol., 173: 180-183.
PubMed - Colegrove, P.M., H.N. Winfield, J.F. Donovan, Jr. and W.A. See, 1999. Laparoscopic practice patterns among North American urologists 5 years after formal training. J. Urol., 161: 881-886.
PubMed - Dagash, H., M. Chowdhury and A. Pierro, 2003. When can I be proficientin laparoscopic surgery? A systematic review of the evidence. J. Pediatr. Surg., 38: 720-724.
PubMed - Duchene, D.A., A. Moinzadeh, I.S. Gill, R.V. Clayman and H.N. Winfield, 2006. Survey of residency training in laparoscopic and robotic surgery. J. Urol., 176: 2158-2166.
PubMed - Feldman, L.S., V. Sherman and G.M. Fried, 2004. Using simulators to assess laparoscopic competence: Ready for widespread use? Surgery, 135: 28-42.
PubMed - Fitzgibbons, Jr., R.J. and V. Puri, 2006. Laparoscopic inguinal hernia repair. Am. Surg., 72: 197-206.
PubMed - Gue, S.S., 1995. Home-made videoscopic trainer for operative laparoscopic surgery. Aust. New Zealand J. Surg., 65: 820-821.
PubMed - Keyser, E.J., A.M. Derossis, M. Antoniuk, H.H. Sigman and G.M. Fried, 2000. A simplified simulator for the training and evaluation of laparoscopic skills. Surg. Endoscopy, 14: 149-153.
PubMed - MacNatt, S.S. and C.D. Smith, 2001. A commuter-based laparoscopic skills assessment device differentiates experienced from novice laparoscopic surgeons. Surg. Endoscopy, 15: 1085-1089.
PubMed - Madan, A.K., C.T. Frantzides, N. Shervin and C.L. Tebbit, 2003. Assessment of individual hand performance in box trainers compared to virtual reality trainers. Am. Surg., 69: 1112-1114.
PubMed - Mughal, M., 1992. A cheap laparoscopic surgery trainer. Ann. Royal Coll. Surg. Engl., 74: 256-257.
PubMed - Risucci, D., A. Geiss, L. Gellman, B. Pinard and J. Rosser, 2001. Surgeon-specific factors in the acquisition of laparoscopic surgical skills. Am. J. Surg., 181: 289-293.
PubMed - Rosser, Jr., J.C., L.E. Rosser and R.S. Savalgi, 1998. Objective evaluation of a laparoscopic surgical skill program for residents and senior surgeons. Arch. Surg., 133: 911-912.
PubMed - Scott, D.J., W.N. Young, S.T. Tesfay, W.H. Frawley, R.V. Rege and D.B. Jones, 2001. Laparoscopic skills training. Am. J. Surg., 182: 137-142.
PubMed - Shalhav, A.L., M.D. Dabagia, T.T. Wagner, M.O. Koch and J.E. Lingeman, 2002. Training postgraduate urologists in laparoscopic surgery: The current challenge. J. Urol., 167: 2135-2137.
PubMed - Shay, B.F., R. Thomas and M. Monga, 2002. Urology practice patterns after residency training in laparoscopy. J. Endourol., 16: 251-256.
PubMed - Stolzenburg, J.U., H. Schwaibold, S.M. Bhanot, R. Rabenalt and M. Do, 2005. Modular surgical training for endoscopic extraperitoneal radical prostatectomy. BJU Int., 96: 1022-1027.
PubMed - Stolzenburg, J.U., R. Rabenalt, M. Do, L.C. Horn and E.N. Liatsikos, 2006. Modular training for residents with no prior experience with open pelvic surgery in endoscopic extraperitoneal radical prostatectomy. Eur. Urol., 49: 491-500.
PubMed - Tang, B., G.B. Hanna and A. Cuschieri, 2005. Analysis of errors enacted by surgical trainees during skills training courses. Surgery, 138: 14-20.
PubMed - Wang, D.S. and H.N. Winfield, 2004. Survey of urological laparoscopic practice patterns in the Midwest. J. Urol., 172: 2282-2286.
PubMed