
Mustafa Abdo Saif Dehwah
College of Life Science, Central China Normal University, Wuhan 430079, China
Zhang Shuang
College of Life Science, Central China Normal University, Wuhan 430079, China
Qing-Yang Huang
College of Life Science, Central China Normal University, Wuhan 430079, China
International Journal of Osteoporosis and Metabolic Disorders
Year: 2008 | Volume: 1 | Issue: 1 | Page No.: 1-7







ABSTRACT
Type 2 diabetes mellitus (T2DM) is a complex disease, as well as one of the world`s most common inherited diseases and a serious international health risk accounting for ~90-95% of all diabetes syndromes. It is characterized by defects in both insulin secretion and action. The prevalence of the disease is increasing and the World Health Organization (WHO) estimates suggest that by 2025 there will be 300 million affected people worldwide. Numerous reports suggesting a substantial genetic contribution to the susceptibility of T2DM and the ACE gene is an important candidate gene for T2DM. So we conducted a case-control association study among 249 T2DM patients and 114 controls with sib-pair and random case-control designs, to investigate the association between ACE gene insertion/deletion (I/D) polymorphism and T2DM in Han Chinese in Hubei. Genotyping for the ACE gene I/D polymorphism was performed by using PCR method. The result showed that the I allele and II genotype were found to be associated with type 2 diabetes in this study population.
PDF Abstract XML References Citation
How to cite this article
Mustafa Abdo Saif Dehwah, Zhang Shuang and Qing-Yang Huang, 2008. The Association Between ACE Gene I/D Polymorphism and Type 2 Diabetes
in Han Chinese in Hubei. International Journal of Osteoporosis and Metabolic Disorders, 1: 1-7.
DOI: 10.3923/ijom.2008.1.7
URL: https://scialert.net/abstract/?doi=ijom.2008.1.7
DOI: 10.3923/ijom.2008.1.7
URL: https://scialert.net/abstract/?doi=ijom.2008.1.7
INTRODUCTION
Type 2 diabetes is a complex disease accounting for ~90-95% of all diabetes syndromes. It is characterized by chronic hyperglycemia resulting from pancreatic β-cell dysfunction and insulin resistance. The prevalence of the disease is increasing and the World Health Organization (WHO) estimates suggest that by 2025 there will be 300 million affected people worldwide (King et al., 1998). Despite numerous reports suggesting a substantial genetic contribution to the susceptibility of type 2 diabetes, no major susceptibility genes have been identified so far (McCarthy and Menzel, 2001). The Angiotensin-Converting Enzyme (ACE) plays an important role in the Rennin-Angiotensin System (RAS), by catalyzes the conversion angiotensin 1 to vasoconstrictor angiotensin 2 in liver and inactivates vasodilator bradykinin in many tissues (Costerousse et al., 1997). RAS may play an important role in diabetic complications, blood pressure regulation and acts a key regulator of sodium homeostasis. One of the (RAS) genes is gene encoding the ACE, which may be associated with diabetic nephropathy. ACE was first isolated in 1956 as a hypertensin-converting enzyme and exists in two distinct forms. The somatic form of ACE is present on the endothelial surface of the lungs and on brush-bordar membranes of kidney, intestine, placenta and choroids plexus and the germinal form, which is found exclusively in testis, plays a crucial role in fertility. Both forms of ACE function at the cell surface as ectoenzymes, where they hydrolyze circulating peptides. ACE is type 1 transmembrane protein that can be cleaved to generate a secreted form in vivo and in a cell culture (Skeggs et al., 1956). The human angiotensin converting enzyme gene is located in chromosome 17q23 with 25 introns and 26 exons; exons 1-12 encode fore the amino domain, exons 13-26 encode fore the carboxyl domain. The gene has been described with an insertion /deletion (I/D) polymorphism, characterized by the presence (insertion) or absence (deletion) of a 287 Alu-repeat sequence inside intron 16, therefore three genotypes were found (DD, II homozygotes and ID heterozygote). This polymorphism accounts fore a large proportion of the variability of serum ACE activity (fore DD genotypes having the highest and II genotypes having the lowest ACE activity) (Rigat et al., 1990). Additionally, there is also an association between the D allele and higher plasma levels of ACE, which seems to be associated with diabetic complications (Marre et al., 1997). ACE gene I/D polymorphism have been suggested to be associated with coronary heart disease and nephropathy in type 2 diabetic patients (Huang et al., 1998; Fujisawa et al., 1998). Association studies of ACE I/D polymorphism and type 2 diabetes in various populations have yielded conflicting results (Bengtsson et al., 1999; Hsied et al., 2000). ACE gene (I/D) polymorphism has been found to be associated with metabolic syndrome in Chinese patients with type 2 diabetes (Lee et al., 2002).
This study was conducted to investigate the association between insertion/deletion (I/D) polymorphism of ACE and type2 diabetes in Han Chinese in Hubei.
MATERIALS AND METHODS
Patients Selection and Clinical Investigation
This study was conducted from Mar 2006 to Oct 2006 and used two experimental designs: Sib-pairs and random case-control designs.
Sib Pairs of T2DM Patients and Controls
We selected 76 sib pairs of T2DM patient-control, the case group consists of 76 T2DM patients (42 males and 34 females), the mean of age was 51.88±11.39 years, the controls group consists of 76 healthy peoples (42 males and 34 females), the mean of age was 50.47±12.00 years. The T2DM entry criteria, in accordance with the 1997 American diabetes association (ADA) announced new diabetes diagnostic criteria: fasting blood glucose (FPG) ≥7.0 mmol L-1 (126 mg dL-1), 2 h postprandial blood glucose ≥11.1 mmol L-1 (200 mg dL-1) for Diabetes patients and FPG < 6.1 mmol L-1 (110 mg dL-1) normal (no diabetic).
Random Case-Control
Random case-control consist of 269 people; the case group consists of 173 T2DM patients (89 males, 84 females), the mean of age was 57.36±13.54 years, the controls group consists of 97 nondiabetic (51 males, 46 females) the mean of age was 52.74±12.59 years. The all subjects were from the Han population in Hubei.
Phenotyping
The weight, height, waist and hip circumference were measured, the body mass index (BMI) [BMI = weight (kg)/height (m2)] and Waist to Hip Ratio (WHR) [WHR = waist (cm)/hip (cm)] were calculated. Determination fasting blood glucose and 2 h postprandial blood glucose by used enzymatic methods; Blood pressure measurement using the recommended guideline for hypertension prevention and control methods; systolic blood pressure (SBP) ≥140 mmHg (1 mmHg = 0.133 kpa) and diastolic blood pressure (DBP) ≥90 mmHg standards for hypertension. This information was completed by the cooperation Hospital.
Genotyping
Genomic DNA was extracted from peripheral blood leukocytes by proteinase K and the phenol chloroform method. To determine the ACE gene I/D polymorphism, a genomic DNA fragment on intron 16 of the ACE gene was amplified by using Polymerase Chain Reaction (PCR) method with a pair of oligonucleotide primers:
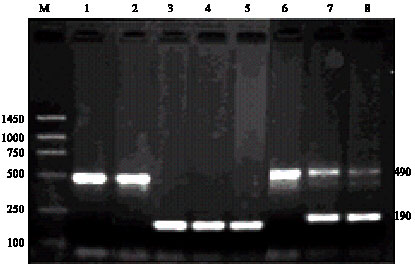 | |
| Fig. 1: | ACE gene I/D polymorphism agarose gel electrophoresis map. Lane M: DiamondTM250bp DNA ladder; Lane 1, 2 and 6: II; Lane 3, 4 and 5: DD; Lane 7 and 8: ID |
The upstream of primer sequence was: 5`-CTG GAG ACC ACT CCC ATC CTT TCT -3` and the downstream was: 5`- GAT GTG GCC ATC ACA TTC GTC AGA T -3` (Shanghai Sangon Biological Engineering Technology and Services Co., Ltd.). The PCR amplification products were obtained using 25 μL reaction system containing; 50 ng μL-1 genomic DNA, ddH2O 15.7 μL, 10xbuffer 2.5 μL, dNTP (10 mmol L-1) 0.5 μL, each of primer sequences (10 μmol L-1) 0.5 μL, MgCL2 (25 mmol L-1) 2 μL and 1U Taq enzyme. On PTC-200 thermal cycler (MJ research company).
After an initial denaturation at 94°C for 5 min, the DNA was amplified by 35 PCR cycles of denaturation at 94°C for 1 min, annealing at 56°C for 1 min and elongation at 72°C for 1 min, followed by a final elongation at 72°C for 10 min. PCR products were separated and sized by electrophoresis on a 2% agarose gel containing ethidium bromide. DNA Marker used Diamond TM 250 bp DNA marker, Voltage 120 V, for 50 min and visualized by Gene Genius Gel imaging system.
Human ACE gene insertion/deletion (I/D) polymorphism, characterized by the presence (insertion) or absence (deletion) of a 287 bp Alu-repeat sequence in Intron 16; the homozygous individuals for insertion allele (II genotype) were identified by the presence of a single 490 bp product, the homozygous individuals for deletion allele (DD genotype) were identified by the presence of a single 190 bp product and the heterozygous individuals` insertion, deletion (ID genotype) was identified by the presence of both 190 and 490 bp products (Fig. 1).
Statistical Analyses
Data are given as the means±standard deviation (SD); the means between two groups were compared by using independent-sample t-test, whereas paired-sample t-test was used for sib-pairs means comparison. The statistical significance of the differences of clinical characteristics between genotypes were compared by analysis of variance (ANOVA). The differences of genotypes distribution and allelic frequencies between two groups were compared with Chi-square analysis. Association analyses were completed by Multiple Logistic regression analysis. A p-value <0.05 was considered statistically significant. All statistical analyses were performed with SPSS11.5 for windows.
RESULTS
Clinical Characteristics of T2DM Group and the Control Group
In all subjects, the results of independent sample t-test analysis between the T2DM patients and the controls group showed that the sex, height, weight, BMI, waist and hip circumference, systolic and diastolic blood pressure were well matched and no significant difference (p>0.05). However, the age, waist to hip ratio (WHR), fasting and postprandial blood glucose of the patients group were significantly higher than the controls group (p<0.05). In the sib pairs of T2DM patients and the controls, the results of the paired sample t-test analysis showed that the sex, height, weight, hip and waist circumference, BMI, waist-hip ratio, systolic and diastolic blood pressure were matched as well as no significant difference (p>0.05), however, fasting and postprandial blood glucose in the T2DM patients were significantly higher than controls group (p<0.05). Moreover, in T2DM patients and unrelated controls, the results showed that the sex, height, weight, BMI, waist circumference, systolic and diastolic blood pressure were matched and no significant difference (p>0.05), however, the age, hip circumference, WHR, fasting and postprandial blood glucose in T2DM patients were significantly higher than controls group (p<0.05). Also in the analysis of the association between I/D polymorphism genotypes and the clinical characteristics in T2DM patients and controls group, the result of ANOVA test showed that, in both T2DM patients and controls group were no significant association between I/D polymorphism genotypes and the clinical characteristics (p>0.05) except in T2DM patients, the age and waist-hip ratio of DD genotype individuals were significantly higher trend than that of each II and ID genotypes individuals, but did not reach to statistical significance (p = 0.057, 0.052, respectively), probably, because of the small number of the subjects.
ACE Gene I/D Polymorphism Genotypes Distribution and Allelic Frequencies
The ACE gene I/D polymorphism genotypes and allele frequencies distribution were found to be in Hardy-Weinberg equilibrium, in the patients group and controls group (p>0.05). In all subjects, the Chi-square test showed, that the genotypes and allelic frequencies distribution of the ACE gene I/D polymorphism between T2DM patients and controls group were significantly different, namely, the II genotype and I allele frequencies distribution were significant higher in type 2 diabetes patients than controls group (p<0.05) (Table 1). However, in sib pairs sample and sample of T2DM patients and unrelated controls, the Chi-square test showed that there was no significant difference of the ACE gene I/D polymorphism genotypes and allelic frequencies distribution between the T2DM patients and the controls group (p>0.05) (Table 2 and 3, respectively).
| Table 1: | ACE gene I/D polymorphism genotypes and allelic frequencies distribution in all subjects |
 | |
| *p<0.05 | |
| Table 2: | ACE gene I/D polymorphism genotypes and allelic frequencies distribution in sib pairs of T2DM patient and controls |
 | |
| Table 3: | ACE gene I/D polymorphism genotypes and allelic frequencies distribution in T2DM patients and unrelated controls |
 | |
| Table 4: | Multivariate logistic regressions of risk factors of T2DM |
 | |
| *p<0.05 | |
Multivariate Logistic regression analysis for all subjects showed that the age and WHR were independent risk factors for type 2 diabetes (p<0.05), but the I/D polymorphism was not an independent risk factor for type 2 diabetes in this study population (Table 4).
DISCUSSION
Proteins of the renin-angiotensin system are involved in regulation of arterial blood pressure and local hemodynamics in tissues (Corvol et al., 1997). The activity of this system is regulated by the rate of angiotensinogen production and the activities of renin and Angiotensin-Converting Enzyme (ACE). ACE is a key element of the renin-angiotensin system; it not only converts angiotensin 1 into angiotensin 2, but also inactivates the vasodilator peptide bradykinin. Studies on the use of ACE inhibitors to lower coronary heart disease risk showed a reduction in progression of impaired glucose tolerance to type 2 diabetes by 25-30% (Stephens et al., 2005). The insertion/deletion polymorphism of ACE gene was detected in 1990 (Rigat et al., 1992). In the previous study on the Taiwan Chinese population, the association between the ACE gene I/D polymorphism and the risk of T2DM was not found (Chuang et al., 1997). In the Swedish population, conversely, allele D was found to be associated with an increased risk of T2DM (but only in hypertensive subjects) (Bengtsson et al., 1999). Also other studies showed that the frequency of ACE gene DD genotype was increased in to type 2 diabetes patients than controls group Taiwanese (Hsied et al., 2000), Caucasian (Stephens et al., 2005), northern Chinese population (Feng et al., 2002) and population-based Japanese (Daimon et al., 2003). In present study, the two experimental designs: sib-pairs and random case-control designs were used to investigate the association between ACE gene I/D polymorphism and type 2 diabetes in Han Chinese in Hubei. The result showed that, in sample of T2DM patients and unrelated controls and sib-pairs sample, there were no significant differences in genotypes and allelic frequencies distribution of I/D polymorphism between T2DM patients and controls group (p>0.05), however, in all subjects sample the frequencies of II genotypes and I allele in T2DM patients were significantly higher than controls group (I: 63.1% vs 44.3%, p<0.05; II: 42.6% vs 27.2%, p<0.05). Thus, the II genotype and I allele were associated with risk for type 2 diabetes in this study population, the result is in agreement with previous study in the Chuvash population Miloserdova et al., 2001). In this study also the results of ANOVA analysis showed that in both T2DM patients and controls group no significant association between ACE gene I/D and clinical characteristics (p> 0.05), except in T2DM patients, the age and waist-hip ratio of DD genotype individuals were significantly higher trend than that of each II and ID genotypes individuals but did not reach to statistical significance (p = 0.057, 0.052, respectively), probably, because of the small number of the subjects. Multiple Logistic regression analysis of all subjects indicated that the age and waist-hip ratio (not the I/D polymorphism) were an independent risk factors for type 2 diabetes in the study population.
CONCLUSIONS
This study detected that the insertion allele I and genotype II were significantly associated with risk for type 2 diabetes in all subjects sample, so that its reasonable to expect the I allele and II genotype of I/D polymorphism may be associated with type 2 diabetes in Han Chinese in Hubei. This study also showed that the age and waist-hip ratio are independent risk factors for type 2 diabetes in this study population. Further studies will be required to confirm and elucidate these findings.
REFERENCES
- Bengtsson, K., M. Orho-Melander, U. Lindblad, O. Melander, E. Bog-Hansen, J. Ranstam, L. Rastam and L. Groop, 1999. Polymorphism in the angiotensin converting enzyme but not in the angiotensinogen gene is associated with hypertension and type 2 diabetes: The Skaraborg hypertension and diabetes project. J. Hypertens., 11: 1569-1575.
PubMedDirect Link - Chuang, L.M., K.C. Chiu, F.T. Chiang, K.C. Lee, H.P. Wu, B.J. Lin and T.Y. Tai, 1997. Insertion/deletion polymorphism of the Angiotensin I-Converting Enzyme gene in patients with hypertension, non-insulin-dependent diabetes mellitus and coronary heart disease in Taiwan. Metabolism, 10: 1211-1214.
CrossRef - Corvol, P., F. Soubrier and X. Jeunemaitre, 1997. Molecular genetics of the renin-angiotensin- aldosterone system in human hypertension. Pathol. Biol., 45: 229-239.
PubMedDirect Link - Costerousse, O., S. Danilov and F. Alhenc-Gelas, 1997. Genetics of angiotensin I-converting enzyme. Clin. Exp. Hypertens., 19: 659-669.
Direct Link - Daimon, M., T. Oizumi, T. Saitoh, W. Kameda, A. Hirata, H. Yamaguchi, H. Ohnuma, M. Igarashi, M. Tominaga and T. Kato, 2003. The D allele of the angiotensin-converting enzyme insertion/deletion (I/D) polymorphism is a risk factor for type 2 diabetes in a population-based Japanese sample. Endocrine J., 50: 393-398.
PubMedDirect Link - Feng, Y., T. Niu, X. Xu, C. Chen, Q. Li, R. Qian, G. Wang and X. Xu, 2002. Insertion/deletion polymorphism of the ACE gene is associated with type 2 diabetes. Diabetes, 51: 1986-1988.
PubMedISIDirect Link - Fujisawa, T., H. Ikegami, Y. Kawaguch, Y. Yamada, H. Ueda and M. Shintani et al., 1998. Meta-analysis of association of insertion/deletion polymorphism of angiotensin I-converting enzyme gene with diabetic nephropathy and retinopathy. Diabetologia, 41: 47-53.
Direct Link - Hsied, M.C., S. Lin, T. Hsieh, C. Hsu, H. Chen, S. Shin and J.H. Tsai, 2000. Increased frequency of angiotensin-converting enzyme DD genotype in patients with type 2 diabetes in Taiwan. Nephrol. Dial. Transplant., 15: 1008-1013.
Direct Link - Huang, X.H., V. Rantalaiho, O. Wirta, A. Pasternack, T. Koivula, T.P. Hiltunen, T. Nikkari and T. Lehtimaki, 1998. Angiotensin-converting enzyme gene polymorphism is associated with coronary heart disease in non-insulin-dependent diabetic patients evaluated for 9 years. Metabolism, 47: 1258-1262.
Direct Link - King, H., R.E. Aubert and W.H. Herman, 1998. Global burden of diabetes, 1995-2025: Prevalence, numerical estimates and projections. Diabetes Care, 21: 1414-1431.
CrossRefPubMedDirect Link - Lee, Y.J. and J.C.R. Tsai, 2002. ACE gene insertion/deletion polymorphism associated with 1998 world health organization definition of metabolic syndrome in Chinese type 2 diabetes patients. Diabetes Care, 25: 1002-1008.
PubMedDirect Link - Marre, M., X. Jeunemaitre, Y. Gallois, M. Rodier, G. Chatellier et al., 1997. Contribution of genetic polymorphism in the renin angiotensin system to the development of renal complications in insulin dependent diabetes. Genetique de la nephropathie diabetique (GENEDÌAB) study group. J. Clin. Acenvest., 99: 1585-1595.
Direct Link - McCarthy, M. and S. Menzel, 2001. The genetics of type 2 diabetes. Br. J. Clin. Pharmacol., 51: 195-199.
CrossRefDirect Link - Miloserdova, O.V., P.A. Slominsky, I.V. Mauyanov, D.S. Markov, M.I. Balabolkin and S.A. Limborska, 2001. Association between the insertion/deletion polymorphism of the angiotensin-converting enzyme gene and angiopathy in patients with non-insulin dependent diabetes mellitus in Chuvash Republic. Russian J. Genet., 1: 98-101.
CrossRefDirect Link - Rigat, B., C. Hubert, F. Alhenc-Gelas, F. Cambien, P. Corvol and F. Soubrier, 1990. An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J. Clin. Invest., 86: 1343-1346.
CrossRefPubMedDirect Link - Rigat, B., C. Hubert, P. Corvol and F. Soubrier, 1992. PCR detection of the insertion/deletion polymorphism of the human Angiotensin-Converting Enzyme Gene (DCP1) (Dipeptidyl Carboxypeptidase 1). Nucl. Acids Res., 20: 1433-1433.
Direct Link - Stephens, J.W., S.S. Dhamrait, J.A. Cooper, J. Acharya, G.J. Miller, S.J. Hurel and S.E. Humphries, 2005. The D allele of the ACE I/D common gene variant is associated with type 2 diabetes mellitus in Caucasian subjects. Mol. Genet. Metab., 84: 83-89.
CrossRefPubMedDirect Link