
A.A. Taheraghdam
Department of Neurology, Tabriz University (Medical Sciences), Tabriz, Iran
H. Amiri
Department of Emergency Medicine, Tehran University of Medical Sciences, Tehran, Iran
H. Shojaan
Department of Internal Medicine, Tabriz University (Medical Sciences), Tabriz, Iran
S. Shamsvahdati
Department of Emergency Medicine, Tabriz University (Medical Sciences), Tabriz, Iran
Y. Houshyar
Physical Medicine and Rehabilitation Research Center, Tabriz University (Medical Sciences), Tabriz, Iran
Pakistan Journal of Biological Sciences
Year: 2011 | Volume: 14 | Issue: 12 | Page No.: 682-687







ABSTRACT
Inflammation is thought to play a significant role in the underlying pathophysiology of migraine headaches which could be controlled by corticosteroids. The present study was conducted to determine and compare the pain relieving effect of dexamethasone versus morphine on patients with acute migraine headache. During this double blinded clinical trial study, 190 patients who met the International Headache Society definition of acute migraine headache were evaluated at emergency department of Tabriz Imam Reza Hospital. After giving informed consent, patients were randomly enrolled into two groups: Receiving either 8 mg dexamethasone (group A) or 0.1 mg kg-1 morphine (group B) intravenously. Severity of the headache was determined using Visual Analog Scale (VAS) scoring method at baseline (VAS-A), 10 min (VAS-B), 60 min (VAS-C) and 24 h (VAS-D) after intervention. The mean age of patients was 44.17±16.20 years, 61.57% male and 38.43% female. The mean of VAS-A and VAS-B scores was not statistically different between two groups (p = 0.236 and p = 0.481), but the mean of VAS-C and VAS-D scores in the group A were significantly lower than the group B (p = 0.017, p = 0.010). In long-term (1 h and 24 h after administration), dexamethasone reduces the severity of acute migrant headache more than morphine.
PDF Abstract XML References Citation
Received: August 13, 2011;
Accepted: October 26, 2011;
Published: November 17, 2011
How to cite this article
A.A. Taheraghdam, H. Amiri, H. Shojaan, S. Shamsvahdati and Y. Houshyar, 2011. Intravenous Dexamethasone Versus Morphine in Relieving of Acute Migraine Headache. Pakistan Journal of Biological Sciences, 14: 682-687.
DOI: 10.3923/pjbs.2011.682.687
URL: https://scialert.net/abstract/?doi=pjbs.2011.682.687
DOI: 10.3923/pjbs.2011.682.687
URL: https://scialert.net/abstract/?doi=pjbs.2011.682.687
INTRODUCTION
A migraine headache is of a common and disabling compliant and diagnosis among adults who come to emergency ward demanding medical intervention. Surveys shows a prevalence of 6-17% in the general population; 6% of men and 15-17% of women experience migraine headaches (Stewart et al., 1994).
Most of patients with migraine headaches experience repeated episodes of acute attack which urges patients to come emergency department for reliving treatment. Majority of patients is treated with oral or intravenous (IV) non-steroidal anti-inflammatories (e.g., ketorelac, ibuprofen, etc.), 5-HT receptor antagonists (Colman et al., 2004a), dopamine antagonists, dihydroergotamine, topiramate, sodium valproate, propranolol, tricyclic antidepressants, IV fluids and IV narcotic analgesics (Bavrasad et al., 2010; Ghasami and Beigi, 2009; Pryse-Phillips et al., 1997; Rafieian-Kopaei et al., 2005).
Most of recent studies have been suggested that treatment of acute migraine headache does not properly address the underlying pathophysiologic inflammatory cascade (Arulmozhi et al., 2006; Longoni and Ferrarese, 2006; Sarchielli et al., 2006). To control inflammatory cascade, attempts are focused on suppressing prostaglandin production by anecdotal use of corticosteroids (Silberstein et al., 2005). Afterward, there are unfortunately a few investigations evaluating corticosteroid therapeutic approach. After introducing corticosteroids as a therapeutic approach for reducing relapse of migraine headaches, only two randomized controlled trials have demonstrated a large benefit of corticosteroids on migraine relapse (Baden and Hunter, 2006; Innes et al., 1999). However, there is a conflicting data about the use of systemic corticosteroids for treating migraine headache (Blumenthal et al., 2003; Colman et al., 2004b; Vinson, 2002). Systematic reviews and Meta analysis have not provided significant and useful results around this topic yet. There is a varying recommendations for systemic corticosteroid therapy; In base of Canadian guidelines, dexamethasone is used as the fourth-line of treatment in case of resistant migraine attacks (Pryse-Phillips et al., 1997). In contrast, other guidelines recommend dexamethasone as a last therapeutic option for status migranosis (Silberstein, 2000). The use of dexamethasone therapy is not common in emergency departments of North American (Colman et al., 2004a).
Most of the studies carried out clinical trials which compared dexamethasone with placebo or added dexamethasone to emergency ward cocktail for migraine therapy. However, there is no definite evidence regarding the effect of dexamethasone on acute episode of migraine headache in comparison to narcotics like morphine. The present study was conducted to determine and compare the pain relieving effect of dexamethasone vs. morphine on patients with acute migraine headache.
MATERIALS AND METHODS
The present study was a prospective, randomized, double-blinded clinical trial was done in emergency ward of Tabriz Imam Reza Hospital from September 2008 to May 2009.
Study population and sampling criteria: Patients who meet inclusion criteria were enrolled into the study with age from 18 to 65 years. These patients came to emergency ward with a chief complaint of “exacerbation of migraine headache”. Symptoms of this disease consistent with the International Headache Society (IHS) criteria for a migraine episode with and without aura (Headache Classification Committee of the International Headache Society, 1988). Treatment regimen should be consisted of IV medications.
Exclusion criteria were that, the patient having a positive pregnancy test with active peptic ulcer disease/history of gastrointestinal bleeding within the past years. Secondly all the patients with diabetes, other metabolic syndrome, allergy to corticosteroids and fever are also excluded. Other reasons of exclusion were acute neurological disorder (stroke symptoms, hypertensive emergency, or symptoms to suggest meningitis or infection), history of familial periodic hypokalemia and immune-suppressed. Patients with the following indications in drug history were also excluded: already receiving corticosteroids, received steroids during the last 30 days, intake the codeine during recent week. Furthermore, refusal/inability to give informed consent and suspicion for narcotic-seeking behavior were among exclusion criteria. Patients were permitted to be enrolled only once in the study.
One hundred and ninety patients met all inclusion criteria were allowed to participate in this study. All participants were given informed written consent and study protocol approved by Ethics Committee of Tabriz University of Medical Sciences (TUMS) which was in compliance with Helsinki declaration.
Study design: After enrollment, establishment of IV access and administration of standard care therapies, patients were assigned a study number and corresponding study packet which were randomly allocated, based on a predetermined randomization schedule. In base of study package, patients were randomly enrolled into two groups: receiving either 8 mg dexamethasone (group A) or 0.1 mg kg-1 morphine (group B), intravenously.
Measuring the severity of headache: The severity of pain was measured by application of a modified Visual Analog Scale (VAS) scoring method (Lines et al., 2001). A VAS is a measurement instrument that tries to measure a characteristic or attitude that is believed to range across a continuum of values and cannot easily be directly measured. For example, the amount of pain that a patient feels ranges across a continuum from none to an extreme amount of pain. From the patient's perspective, VAS spectrum appears continuous and there is not an undefined interval in description of headache severity as what presents in categorization to none, mild, moderate and severe. It was to capture this idea of an underlying continuum that the VAS was devised. Operationally, a VAS is usually a horizontal line, 10 cm in length, anchored by word descriptors at each end, as illustrated in Fig. 1. The patient marks on the line the point that they feel represents their perception of their current state. The VAS score is determined by measuring in millimeters from the left hand end of the line to the point that the patient marks. Severity of the headache was determined using visual analog scale (VAS) scoring method at baseline (VAS-A), 10 min (VAS-B), 60 min (VAS-C) and 24 h (VAS-D) after intervention.
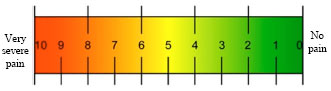 | |
| Fig. 1: | Illustration of Visual Analog Scale (VAS). The VAS is usually assessed using a horizontal line with 10 cm length as above |
Statistical analysis: Statistical analysis was performed using the SPSS Statistical Package version 13.0 (SPSS Inc, Chicago, Ill, USA). The results are shown as Mean±SD. Distribution of variables was determined by Skewness, Kurtosis and Kolmogorov-Smirnov Z test (Shorak and Wellner, 1986). General linear model repeated measures analysis was applied to evaluate the significance of changes after receiving treatment in each group. To assess the differences among the evaluation times (among VAS-A, VAS-B, VAS-C and VAS-D), paired sample t-test were used and the differences between the group A and B were studied using independent sample t-test. A p-value less than 0.05 were considered significant.
RESULTS
Finally, data of 190 patients with acute migraine headache was analyzed.
One-way repeated-measures analysis of variance showed significant changes in the mean VAS scores of group A (dexamethasone intervention) during the study period (Wilks’ Lambda = 0.439, F (2, 28) = 10.657, p<0.001, multivariate partial eta squared = 0.638; Fig. 2). The mean VAS score was significantly decreased after 10 min of dexamethasone therapy. Comparison of 60th min and 24th hour of dexamethasone therapy showed that the VAS score was also significantly reduced. Finally, the VAS score determined 60 min and 24 h after receiving dexamethasone were significantly lower than the baseline score (p<0.001, p<0.001).
One-way repeated-measures analysis of variance showed significant changes in the mean VAS scores of group B (morphine intervention) during the study period (Wilks’ Lambda = 0.526, F (2, 28) = 9.950, p<0.001, multivariate partial eta squared = 0.611; Fig. 2). The mean VAS score was significantly decreased after 10 minutes of morphine therapy. Comparison of 60th minutes and 24th hours of morphine therapy showed that the VAS score was also significantly reduced. Finally, the VAS score determined 60 min and 24 h after receiving morphine were significantly lower than the baseline score (p<0.001, p<0.001).
The mean age of group A and B was not statistically different (p = 0.100). Comparison of dexamethasone and morphine effects in relieving headache at different studied times is shown in Table 1.
| Table 1: | Comparison of age and dexamethasone versus morphine effects in relieving headache at different studied times. |
 | |
| SD: Standard Deviation, LBP: Low back pain. VAS-A: Visual analog scale at baseline, VAS-B: Visual analog scale 10 min after intervention, VAS-C: Visual analog scale 60 min after intervention, VAS-D: Visual analog scale 24 h after intervention | |
 | |
| Fig. 2: | The serial scores of Visual Analog Scale (VAS) in patients with acute migraine headache at baseline (before intervention), 10 min, 60 min and 24 h after dexamethasone (group A) and morphine (group B) therapy. After administration dexamethasone, both groups' VAS scores were significantly reduced during study duration (p<0.001) |
The mean of VAS-A and VAS-B scores was not statistically different between two groups (p = 0.236 and p = 0.481). However, the mean of VAS-C and VAS-D scores in the group A were significantly lower than the group B (p = 0.017, p = 0.010).
The gender distribution and VAS scores are shown according to their studied group and gender in Table 2. Distribution of genders was not different between two groups (p = 0.089). Also, there was not significant difference between males and females regarding the age, VAS-A, VAS-B, VAS-C and VAS-D scores (p = 0.102, p = 0.271, p = 0.355, p = 0.264 and p = 0.710, respectively).
| Table 2: | Characteristics and VAS scores of study population according to their studied group and gender |
 | |
| SD: Standard Deviation, LBP: Low back pain. VAS-A: Visual analog scale at baseline, VAS-B: Visual analog scale 10 min after intervention, VAS-C: Visual analog scale 60 min after intervention, VAS-D: Visual analog scale 24 h after intervention | |
DISCUSSION
The present study showed that dexamethasone reduced the severity of acute migrant headache more than morphine at 1 h and 24 h check points after administration. To the best of our knowledge, this is the first randomized clinical trial compared the pain relieving effect of dexamethasone with morphine in patients with acute migraine headache discharged from the emergency department.
A recent considerations suggest that current therapeutic approaches to acute migraine do not adequately address the inflammatory cascade coincide with an acute attack (Arulmozhi et al., 2006; Longoni and Ferrarese, 2006; Sarchielli et al., 2006). Attempts to suppress prostaglandin production have led to the anecdotal use of corticosteroids in an attempt to mitigate inflammation (Silberstein et al., 2005). However, only a few investigators have investigated this therapeutic approach. The use of parenteral corticosteroids had been proposed as a method to reduce relapses and at least two randomized controlled trials have demonstrated a large benefit of treatment with corticosteroids (Baden and Hunter, 2006; Innes et al., 1999). However, the existing literature documenting the use of systemic corticosteroids in the treatment of migraine headache is conflicting (Blumenthal et al., 2003; Colman et al., 2004b; Vinson, 2002) and systematic reviews have not yet provided a clear answer.
Prior to the present study, nine clinical trials have studied the effect of corticosteroids on acute migraine headache (Baden and Hunter, 2006; Beveridge, 1998; Donaldson et al., 2008; Dong et al., 2007; Fiesseler et al., 2011; Friedman et al., 2007; Innes et al., 1999; Kelly et al., 2008; Rowe et al., 2008; Silberstein, 2000).
During a multi-center clinical trial, Innes et al. (1999) demonstrated that 24 mg of dexamethasone intravenously decreased the incidence of severe recurrent headache after emergency ward treatment. Baden and Hunter (2006). study on “benign headaches” at multiple military base hospital emergency departments demonstrated that only 9.7% (3/31) of those receiving IV dexamethasone (10 mg) had headache recurrence, whereas those receiving placebo had a 58.3% (14/24) recurrence rate (p = 0.001). These two studies results in reducing relapsing rate were in part consistent with what was shown by the present study in reducing severity of migraine headache.
Donaldson et al. (2008) performed a multi-center clinical trial utilizing 24 mg of dexamethasone intravenously in 115 migraine patients meeting the IHSC. During 3 days follow-up, 45% of the placebo group had recurrence of migraine, compared with 35% in the dexamethasone arm (p = 0.68). Donaldson was unable to show a significant decrease in migraine recurrence with 24 mg of dexamethasone. In another clinical trial, Rowe et al. (2008) were unable to demonstrate a significant reduction in migraine headache recurrence in their multi-center clinical trial. Administration of 15 mg of parenteral dexamethasone resulted in pain recurrence at 48-72 h in 14/64 (22%) and 20/62 (32%) patients in the dexamethasone and placebo arm, respectively (p = 0.19). Fiesseler et al. (2011) did not find a statistically significant decrease in headache recurrence in patients treated with steroids for migraine headaches. Enrollees received 10 mg, intravenous dexamethasone. Of the 173 patients with completed follow-up, 14/64 (22%) in the dexamethasone group and 26/82 (32%) in the placebo arm had recurrent headaches at 48-72 h, respectively (p = 0.21). These three studies have failed to demonstrate an effect for dexamethasone in improving recurrence of migraine headache, in contrast to the present study findings.
Collectively, all of studies suggest a moderate effect or somewhat ineffectiveness of dexamethasone on migraine headache relapse following discharge. None of these studies evaluated the possible effect of dexamethasone on acute migraine severity (Baden and Hunter, 2006; Beveridge, 1998; Donaldson et al., 2008; Dong et al., 2007; Fiesseler et al., 2011; Friedman et al., 2007; Innes et al., 1999; Kelly et al., 2008; Rowe et al., 2008; Silberstein, 2000).
A very similar clinical trial studied the effect of dexamethasone versus dihydroergotamine in controlling migraine headache showed that the severity of headaches in both of dexamethasone and dihydroergotamine groups were reduced 10 and 30 min after administration of drugs. This study revealed that there was no difference for severity of headache between dexamethasone and dihydroergotamine 10 and 30 min after IV injection of drugs. However, some patients in dihydroergotamine group got side effects, while no side effect was reported by patients in dexamethasone group (Jivad and Rafieian-Kopaei, 2005). The results of this study comparing dexamethasone versus dihydroergotamine were consistent with the present study results which assessed dexamethasone versus morphine in reducing severity of migraine headache.
Inflammation is an essential underlying etiology in promotion and development of migraine headache and dexamethasone is a potential anti-inflammatory pharmacologic agent. Hence, the results of both studies were not proposed a relationship between anti-migraine and anti-inflammatory effects of dexamethasone. Reviewing the present study and results of Jivad and Rafieian-Kopaei (2005) revealed and that dexamethasone reduces migraine headache severity as early as 10 min and one h after administration, while this drug anti-inflammatory effects and reducing prostoglandins production were not complete during this time period (Sweetman, 2011). Therefore, how dexamethasone ameliorate migraine headache remains to be clear by further studies.
In another study on 205 patients with migraine headache, dexamethsone effect was compared to placebo (Friedman et al., 2007). Although, researchers found significant benefit in persistent headache relief rates for dexamethasone in their study, they advised that the results should be interpreted cautiously because the finding was a result of subgroup analysis. In addition, these author suggest that data may not be generalizable. Because all subjects in this study received at least 20 mg of metoclopramide and 25 mg of diphenhydramine, the utility of adding dexamethasone to this protocol was tested. Therefore, do not recommend the administration of 10 mg of IV dexamethasone for the ED treatment of acute migraine. Despite the discrepancy in final suggestions between the present and Friedman et al. (2007) study, results are shown dexamethasone effectiveness in reliving migraine headache.
The present study suffers from several limitations warranting further discussion including lack of analysis for interval between began and coming to emergency department, weight adjusted doses of dexamethasone, follow-up for relapse. Furthermore, utilization of standardized ED medication protocols was implemented. It is thought that enrolling physicians with personal treatment regimens would be another limitation of this study. However, medication administration between the two groups was similar and with the double-blind randomized nature of the study, medication treatment differences were likely balanced between groups.
In general, it appears that corticosteroids have a role to play in the treatment of acute migraine and their exact role remains to be determined by demonstrating possible mechanisms. In order to resolve this important question from the perspective of care providers as well as patients, larger randomized clinical trials are required.
CONCLUSION
Although the pain reliving effect of dexamethasone was not different from morphine in short-term, dexamethasone relieves and reduces the severity of acute migraine headache more than morphine in long-term. However, a larger trial may be warranted to confirm the present study results.
ACKNOWLEDGMENT
The authors would like to thank Dr. Nariman Nezami for his memorable efforts on the present study.
REFERENCES
- Arulmozhi, D.K., A. Veeranjaneyulu and S.L. Bodhankar, 2006. Migraine: Current therapeutic targets and future avenues. Curr. Vasc. Pharmacol., 4: 117-128.
PubMedDirect Link - Baden, E.Y. and C.J. Hunter, 2006. Intravenous dexamethasone to prevent the recurrence of benign headache after discharge from the emergency department: A randomized, double-blind, placebo-controlled clinical trial. Can. J. Emerg. Med., 8: 393-400.
PubMedDirect Link - Bavrasad, R., S.E.M. Nejad, A.R. Yarahmadi, S.I. Sajedi and F. Rahim, 2010. Assessment of the middle dose of topiramate in comparison with sodium valproate for migraine prophylaxis: A randomized-double-blind study. Int. J. Pharmacol., 6: 670-675.
CrossRefDirect Link - Beveridge, R., 1998. CAEP issues. The Canadian triage and acuity scale: A new and critical element in health care reform. J. Emerg. Med., 16: 507-511.
PubMedDirect Link - Blumenthal, H.J., M.A. Weisz, K.M. Kelly, R.L. Mayer and J. Blonsky, 2003. Treatment of primary headache in the emergency department. Headache, 43: 1026-1031.
PubMedDirect Link - Headache Classification Committee of International Headache Society, 1988. Classification and diagnostic criteria for headache disorders, cranial neuralgia and facial pain. Cephalalgia, 8: 1-96.
PubMed - Colman, I., M.D. Brown, G.D. Innes, E. Grafstein, T.E. Roberts and B.H. Rowe, 2004. Parenteral metoclopramide for acute migraine: meta-analysis of randomised controlled trials. Br. Med. J., 329: 1369-1373.
CrossRefPubMedDirect Link - Colman, I., A. Rothney, S.C. Wright, B. Zilkalns and B.H. Rowe, 2004. Use of narcotic analgesics in the emergency department treatment of migraine headache. Neurology, 62: 1695-1700.
PubMedDirect Link - Donaldson, D., R. Sundermann, R. Jackson and A. Bastani, 2008. Intravenous dexamethasone vs placebo as adjunctive therapy to reduce the recurrence rate of acute migraine headaches: A multicenter, double-blinded, placebo-controlled randomized clinical trial. Am. J. Emerg. Med., 26: 124-130.
CrossRefDirect Link - Dong, S.L., M.J. Bullard, D.P. Meurer, S. Blitz and E. Akhmetshin et al., 2007. Predictive validity of a computerized emergency triage tool. Acad. Emerg. Med., 14: 16-21.
CrossRefPubMedDirect Link - Fiesseler, F.W., R. Shih, P. Szucs, M.E. Silverman and B. Eskin et al., 2011. Steroids for migraine headaches: A randomized double-blind, two-armed, placebo-controlled trial. J. Emerg. Med., 40: 463-468.
CrossRefPubMedDirect Link - Friedman, B.W., P. Greenwald, T.C. Bania, D. Esses and M. Hochberg et al., 2007. Randomized trial of IV dexamethasone for acute migraine in the emergency department. Neurology, 69: 2038-2044.
CrossRefPubMedDirect Link - Ghasami, K. and A.M. Beigi, 2009. Comparison of treatment effect of sodium valprovate, propranolol and tricyclic antidepressants in migraine. Pak. J. Biol. Sci., 12: 1098-1101.
CrossRefPubMedDirect Link - Innes, G.D., I. Macphail, E.C. Dillon, C. Metcalfe and M. Gao, 1999. Dexamethasone prevents relapse after emergency department treatment of acute migraine: A randomized clinical trial. Can. J. Emerg. Med., 1: 26-33.
PubMedDirect Link - Jivad, N. and M. Rafieian-Kopaei, 2005. Is dexamethasone a suitable alternative for dihydroergotamine on migraine attacks? Int. J. Pharmacol., 1: 357-359.
CrossRefDirect Link - Kelly, A.M., D. Kerr and M. Clooney, 2008. Impact of oral dexamethasone versus placebo after ED treatment of migraine with phenothiazines on the rate of recurrent headache: A randomised controlled trial. Emerg. Med. J., 25: 26-29.
CrossRefPubMedDirect Link - Lines, C.R., K. Vandormael and W. Malbecq, 2001. A comparison of visual analog scale and categorical ratings of headache pain in a randomized controlled clinical trial with migraine patients. Pain, 93: 185-190.
PubMed - Longoni, M. and C. Ferrarese, 2006. Inflammation and excitotoxicity: Role in migraine pathogenesis. Neurol. Sci., 27: S107-S110.
CrossRefPubMedDirect Link - Pryse-Phillips, W.E., D.W. Dodick, J.G. Edmeads, M.J. Gawel and R.F. Nelson et al., 1997. Guidelines for the diagnosis and management of migraine in clinical practice. Can. Med. Assoc. J., 156: 1273-1287.
PubMedDirect Link - Rafieian-Kopaei, M., J. Mehvari and H. Shirzadeh, 2005. Different profile of propranolol and amitriptyline effects on migraine prophylaxis. Int. J. Pharmacol., 1: 366-368.
CrossRefDirect Link - Rowe, B.H., I. Colman, M.L. Edmonds, S. Blitz, A. Walker and S. Wiens, 2008. Randomized controlled trial of intravenous dexamethasone to prevent relapse in acute migraine headache. Headache, 48: 333-340.
CrossRefPubMedDirect Link - Sarchielli, P., A. Alberti, A. Baldi, F. Coppola and C. Rossi et al., 2006. Proinflammatory cytokines, adhesion molecules, and lymphocyte integrin expression in the internal jugular blood of migraine patients without aura assessed ictally. Headache, 46: 200-207.
CrossRefPubMedDirect Link - Silberstein, S.D., 2000. Practice parameter: Evidence-based guidelines for migraine headache (an evidence based review). Rep. Qual. Standards Subcommittee Am. Acad. Neurol., 55: 754-762.
PubMed - Silberstein, S.D., R.B. Lipton and N.M. Ramadan, 2005. From migraine mechanisms to innovative therapeutic drugs. Neurology, 64: S1-S3.
Direct Link - Stewart, W.F., A. Shechter and B.K. Rasmussen, 1994. Migraine prevalence. A review of population-based studies. Neurology, 44: S17-S23.
PubMed - Vinson, D.R., 2002. Treatment patterns of isolated benign headache in US emergency departments. Ann. Emerg. Med., 39: 215-222.
CrossRefPubMedDirect Link