
Fatolahzadeh B.
Department of Microbiology, Faculty of Medicine, Tehran University of Medical Sciences, Tehran, Iran
P. Maleknejad
Department of Microbiology, Faculty of Medicine, Tehran University of Medical Sciences, Tehran, Iran
A. Bahador
Department of Microbiology, Faculty of Medicine, Tehran University of Medical Sciences, Tehran, Iran
H. Peeri- Dogaheh
Faculty of Medicine, Ardebil University of Medical Sciences, Ardebil, Iran
M. Y. Alikhani
Faculty of Medicine, Hamedan University of Medical Sciences, Hamedan, Iran
R. Radmanesh-Ahsani
Department of Microbiology, Faculty of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Pakistan Journal of Biological Sciences
Year: 2007 | Volume: 10 | Issue: 1 | Page No.: 107-111







ABSTRACT
Pleural fluid samples from patients with exudative effusion who were diagnosed with tuberculous pleuritis are examined using a new designed primer set based on IS1081 gene (IS1081-PCR) and rpoB-PCR. The PCR results are compared with the results of the sample cultures, using Loewenstein-Jensen (LJ) medium and Ziehl-Neelsen (ZN) staining. Of 78 cases that were confirmed as tuberculous pleuritis by histopathology, supported by sputum culture, biochemical markers (adenosine deaminase, gamma interferon and tumor necrosis factor), radiographic and clinical data, 61 (78.2%) were positive by IS1081-PCR, 43 (55.1%) by rpoB-PCR, 17 (21.7%) by culture and 3 (3.8%) by ZN stain. When IS1081-PCR test results were compared with the confirmed culture, the sensitivity, specificity, positive predictive value and negative predictive value for the IS1081-PCR were 94.1, 55.7, 37.2 and 97.1%, respectively. The corresponding values for the rpoB-PCR were 94.1, 26.2, 26.2 and 94.1%, respectively. When tests results were compare with the confirmed radiographic, histopathology, biochemical markers and clinical diagnosis of tuberculous pleuritis, the IS1081-PCR assay is more sensitive, specific and reliable than both rpoB-PCR assay and culture.
PDF Abstract XML References Citation
How to cite this article
Fatolahzadeh B., P. Maleknejad, A. Bahador, H. Peeri- Dogaheh, M. Y. Alikhani and R. Radmanesh-Ahsani, 2007. Evaluation of Different Primer Sets for the Rapid Diagnosis of Tuberculosis. Pakistan Journal of Biological Sciences, 10: 107-111.
DOI: 10.3923/pjbs.2007.107.111
URL: https://scialert.net/abstract/?doi=pjbs.2007.107.111
DOI: 10.3923/pjbs.2007.107.111
URL: https://scialert.net/abstract/?doi=pjbs.2007.107.111
INTRODUCTION
Pleural tuberculosis (tuberculous pleuritis) is a major, treatable cause of exudative pleural effusion (David et al., 1987). The frequency of pleural effusion in tuberculosis (TB) patients is approximately 31%, worldwide (Ferrer, 1997). However, the epidemiology and demographics of tuberculous pleurisy are changing due to the impact of HIV co-infection and the increasing number of pleural effusions seen as part of re-activation disease (Chakrabarti and Davies, 2006). Pleural involvement may be primary, secondary to pulmonary TB (e.g., miliary TB) or post primary (reactivation) TB pleurisy. Ibrahim et al. (2005) showed that, in contrast to what has been reported in developed countries, Pleural tuberculosis tends to be a primary disease in developing countries and younger age groups are particularly affected.
Among the extrapulmonary presentations of TB, pleural TB is second only to TB lymphadenitis (Villegas et al., 2000).
The diagnosis of pleural TB is generally established by the presence of tubercle bacilli in the sputum, pleural fluid, or pleural biopsy specimen, laboratory culture of the causative organism or the demonstration of granuloma in the pleura by histopathologic examination. Analysis of pleural fluid and pleural biopsy, adenosine deaminase (ADA), gamma interferon (INFγ) and other lymphokines can improve diagnostic efficiency (Philip and Barry, 1994; Sharma and Banga, 2005; Chakrabarti and Davies, 2006). TB pleural effusions are not always easy to diagnose, because the typical features such as presence of a lymphocyte-rich exudative pleural effusion associated with caseous necrotic granuloma in pleural biopsy, positive Ziehl-Neelsen (ZN) stains or Lowenstein-Jensen (LJ) cultures of effusions or tissue samples and cutaneous sensitivity to PPD are not invariably present (Valdes et al., 1998).
Advances in rapid diagnostic methods and direct differentiation of Mycobacteria sp., especially in immunocompromised patients, are urgently needed for the early management and successful treatment of patients and TB control (Ravn et al., 2005; Brown et al., 1999). The sensitivity of culturing methods for the detection of mycobacteria in extrapulmonary tuberculosis is very low (Cheng et al., 2005). Diagnostic assays based on Polymerase Chain Reaction (PCR) dramatically decrease the time required for organism detection. This method has been tested extensively for extrapulmonary tuberculosis (Chakrabarti and Daives, 2006; Ieven and G, 1997; Choi et al., 1996; Scarpellini et al., 1995; Pietrzak et al., 1994; Brisson-Noel et al., 1991). PCR has also been used to detect Mycobacterium tuberculosis (MTB) in pleural fluid samples, with highly variable sensitivity (11 to 81%) in different studies (Cegielski et al., 1997; Kolk et al., 1992; Querol et al., 1995).
Comparatively little work has been focused on the utility of different types of PCR and culture. In this study, we examined two PCR assays (the IS1081- and rpoB-PCR assays) to determine which PCR assay gave better results and whether the PCR of pleural specimens is superior to that of the culture of pleural fluid in detecting MTB. There are multiple copies (five to seven) of the IS1081 gene within the MTB genome. The rpoB gene encompasses the region associated with rifampin resistance in MTB (Kim et al., 2001). Our primary objective in this study was to apply PCR to detect DNA specific for MTB in pleural fluid specimens using a new designed primer set based on IS1081 gene that specific for the mycobacterium complex (De Lassence et al., 1992; Colline and Stephens, 1991) and compare it to the rpoB-PCR assays, pleural fluid cultures using LJ medium and ZN staining.
MATERIALS AND METHODS
In this study, the MgCl2, dNTP, Taq polymerase, 10X PCR buffer were purchased from Fermentas, Canada; the primers were from TIB MOLBIOL, Germany; the tris-HCl, EDTA, lysozyme, proteinase K and SDS were all from Sigma-Aldrich, USA.
Processing of pleural fluid samples: From 2002 to 2005, 78 pleural fluid samples from patients with tuberculosis exudative effusion were received in the Microbiology Laboratory of Tehran University of Medical Sciences (TUMS). Samples were subjected to decontamination with N-acetyl-L-cisteine-NaOH (NALC) (Bahador et al., 2004). The pellets were resuspended in sterile normal saline solution and used for ZN smear, culture and PCR studies.
Loewenstein-jensen culture of pleural fluid samples: Concentrated pleural fluid specimens (0.1 mL) were inoculated into LJ medium and were kept in an incubator for 8 weeks. Bottles were inspected twice a week for visible colonies. Suspicious growth was subjected to ZN staining. Negative cultures were discarded after 8 weeks. Cultures with growth were left under light for 2 h and examined for yellow pigment to identify photochromogenic species.
DNA extraction: DNA extraction was performed by the SDS/lysozyme method (Bahador et al., 2004).
IS1081-PCR: We designed a novel primer set from IS1081 gene by Primer3 program for detection of Mycobacterium tuberculosis complex. The primers specific for IS-1081 (5`-CGAATCAGTTGTTGCCCAAT-3`, 5`-GTTCTTCGGTGCTGGTCAGT-3`) enclosed a 344-bp fragment located at positions 85 to 428 of the IS-1081 gene (GenBank accession number MBBIS1081). Samples were amplified by PCR in 25 μL reaction mixtures containing: 1 μL dNTP (10 mM), 1 μL of each primer (20 pM), 0.25 μL (500 U) Taq polymerase, 1.5 μL MgCl2 (25 mM), 2.5 μL of 10X PCR buffer and 2 μL of DNA template.
The amplification parameters included an initial denaturation at 95°C for 5 min followed by 40 cycles each of denaturation at 95°C for 30 sec, annealing at 56°C for 30 sec and extension at 72°C for 45 sec. The extension step in the 40th cycle was held for 5 min before the samples were detected.
rpoB-PCR: The rpoB assay was performed as described previously (Kim et al., 2001).
The amplified products were detected by gel electrophoresis using 1.5% agarose gel with ethidium bromide.
RESULTS
We tried a new set of PCR primers based on the sequence of the IS1081 insertion element of the M. tuberculosis complex and one primer based on the published nucleotide sequence of rpoB in mycobacteria. Figure 1 shows an example of PCR amplification from a patient sample positive for the M. tuberculosis.
As shown in Table 1, 78 pleural tuberculosis cases were confirmed by histopathology of pleural biopsy specimens, supported by laboratory (sputum culture), biochemical markers like ADA, gamma interferon and tumor necrosis factor, radiographic and clinical data. 17 cases were confirmed by culture and 3 were confirmed by microscopy and 14 were AFB smear-negative and culture-positive.
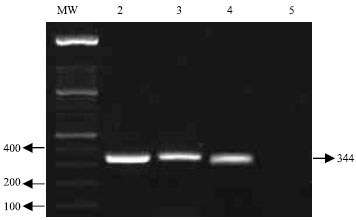 | |
| Fig. 1: | 1.2% Ethidium bromide-stained gel of PCR products. Lane MW: 100 bp molecular size marker; Lane 2: PCR product of IS1081 gene of the H37Rv; Lane 3: rpoB-PCR product of the patient sample; Lane 4: PCR product of IS1081 gene of the patient sample 5: negative control |
| Table 1: | Comparison of culture, ZN, rpoB-PCR and IS1081-PCR |
 | |
The PCR results in Table 1 show that, of 61 patients positive for the IS1081 sequence by the PCR amplification, 3 patients were found positive for acid-fast bacilli using the ZN staining protocol and only 16 were found positive by culture on LJ medium. PCR amplification readily detected the rpoB sequence in 43 out of 78 patient samples. Of 35 patients who were negative using rpoB, 19 patients were found positive for the IS1081 sequence. One of pleural fluid samples had a positive result by rpoB-PCR that was negative for 1081-PCR and was considered to be non-tuberculosis mycobacteria (NTM).
The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of the rpoB-PCR, 1081-PCR and ZN tests performed on the pleural fluid samples from patients compared with culture as gold standard are shown in Table 1. The sensitivity of the mycobacterial DNA detection PCR was 94.1% with the rpoB -PCR and 1081-PCR. The specificity of the rpoB-PCR was 55.7 and 26.2% for other PCR method. The PPV was much lower, with values ranging from 26.2% with the 1081-PCR to 100% with the ZN stain. The NPV of the test ranged from 81.3% for ZN stain to 97.1% for rpoB -PCR. When IS1081-PCR test results were compared with the confirmed radiographic, histopathology, biochemical markers and clinical diagnosis of tuberculous pleuritis, the sensitivity, for the IS1081-PCR and rpoB-PCR were 78.2 and 55.1%, respectively.
DISCUSSION
At present, the most reliable method for the diagnosis of tuberculous pleuritis is the identification of MTB in pleural specimens (Ahmad et al., 1998). Rapid diagnosis and treatment of tuberculous pleuritis is crucial in order to reduce morbidity and mortality caused by untreated tuberculosis. Because the differential diagnosis of exudative pleural effusion is broad, the rapid diagnosis of tuberculous pleural effusion would greatly facilitate the management of these patients. The mean detection time of MTB was 28 days for LJ specimen culture, 40 min for ZN stain and 7 h for PCR.
Theoretically, PCR for the MTB genome should be a highly effective and rapid method for diagnosing tuberculous pleuritis. Using different genomic DNA sequences and extraction methods, MTB-PCR studies of pleural fluid from patients with tuberculosis pleuritis have produced highly variable outcomes, with diagnostic sensitivity ranging from 20 to 81% .This probably reflects the importance of experience, technique and sensitivity in the utilization of this test (Neimark et al., 1996; DeWit et al., 1992; De Lassence et al., 1992; Querol et al., 1995; Kuwano et al., 1995).
Most researchers have reported using insertion element IS6110 primers for direct detection of tuberculosis. Villegas et al. (2000) have evaluated PCR directed toward the IS6110 sequence of MTB, reporting that the IS6110-PCR had a false-negative result in two patients with tuberculous effusion. In the studies of Parandaman et al. (2000) and Villegas et al. (2000) there were 22% false-negative results by PCR with IS-6110 primers. The high number of false negatives using PCR with IS6110 may in part be due to the absence of IS6110 copies in MTB. PCR is positive in 100% of the culture-positive TB pleural fluids (Parandaman et al., 2000), but PCR is positive in only 30-60% of culture-negative pleural fluids. The study of Reechaipichitkul et al. (2000) reveals that the sensitivity and specificity of pleural fluid cultures on LJ medium were 17 and 100%, respectively, whereas the sensitivity and specificity of the pleural fluid PCR-assay of the 16 S-23 S rRNA gene spacer sequences was 50 and 61%, respectively.
We compared the performance of the IS1081-PCR and rpoB-PCR assays for the detection of tuberculosis pleuritis. Our study showed that, using the IS1081-PCR assay, 61 of 78 samples (78.2%) were positive. The rpoB-assay had 43 (55.1%) positives of 78 samples (Table 1). The detection rate of the IS1081-PCR and rpoB-PCR assays differed significantly (78.2% versus 55.1%, respectively, p<0.05). The superior detection rate of the IS1081-PCR could be due to multiple copies (five to seven) of IS1081 within the chromosome of all strains belonging to the M. tuberculosis complex. The ZN staining results of pleural fluid specimens were positive in only 3 patients (3.8%) with tuberculous pleural effusion (Table 1). Of all the samples, only 17 (21.7%) led to a confirmed diagnosis of tuberculous pleuritis based on culture results (Table 1). In pleural fluid specimens, the sensitivity of IS1081-PCR test for diagnosing TB in our study was 78.2%, which was similar to that reported by Querol et al. (1995) (81%) but higher than that reported by Shi et al. (1994) (52.9%).
19 IS1081 PCR-positive samples tested negative in the rpoB-PCR assays (Table 1) indicated that the rpoB-PCR assays have lower detection ability and this could be because there is only one of the rpoB genes in the MTB genome compared to the five to seven copies of IS1081. One IS1081-PCR negative patients in our study that was positive by rpoB-PCR from pleural fluid may be due to an NTM infection. NTM organisms do not have IS1081 gene in their chromosome.
Using PCR, the presence of multiple copies of IS1081 in all strains belonging to MTB complex should be easily detectable in tuberculous patients. The utility of rpoB-PCR for the differential identification of mycobacterial species based on PCR restriction-fragment length polymorphism (PCR-RFLP) is its main advantage over other current procedures available for the direct detection of mycobacteria.
The main limitation of our study is that currently there is no diagnostic test to serve as an adequate “gold standard” to evaluate PCR. Since the culture method has low sensitivity, clinical assessment may be subjective.
In conclusion, the results of the present study show that the PCR assay can successfully be used to detect M. tuberculosis DNA in pleural fluid samples for a more rapid, specific and reliable tuberculous pleuritis diagnosis than the LJ medium culture and ZN staining methods. In this study we demonstrated that the IS1081-PCR assay is more sensitive, specific and reliable than the rpoB-PCR assay.
REFERENCES
- Ahmad, N., A.K. Mohanty, U. Mukhopadhyay and V.K. Batish, 1998. PCR-based rapid detection of Mycobacterium tuberculosis in blood from immunocompetent patients with pulmonary tuberculosis. J. Clin. Microbiol., 36: 3094-3095.
Direct Link - Bahador, A., H. Etemadi, B. Kazemi and R. Ghorbanzadeh, 2004. Comparison of DNA extraction methods for detection of Mycobacterium tuberculosis by PCR. J. Med. Sci., 4: 252-256.
Direct Link - Brisson-Noel, A., C. Aznar and C. Chureau, 1991. Diagnosis of tuberculosis by DNA amplification in clinical practice evaluation. Lancet, 338: 364-366.
Direct Link - Brown, T.J., E.G. Power and G.L. French, 1999. Evaluation of three commercial detection systems for Mycobacterium tuberculosis where clinical diagnosis is difficult. J. Clin. Pathol., 52: 193-197.
Direct Link - Cegielski, J.P., B.H. Devlin, A.J. Morris, J.N. Kitinya, U.P. Pulipaka, L.E.K. Lema and J.L. Wakatare, 1997. Comparison of PCR, culture and histopathology for diagnosis of tuberculous pericarditis. J. Clin. Microbiol., 35: 3254-3257.
Direct Link - Cheng, V.C., W.W. Yew and K.Y. Yuen, 2005. Molecular diagnostics in tuberculosis. Eur. J. Clin. Microbiol. Infect. Dis., 24: 711-720.
CrossRef - Choi, Y.J., Y. Hu and A. Mahmood, 1996. Clinical significance of a polymerase chain reaction assay for the detection of Mycobacterium tuberculosis. Am. J. Clin. Pathol., 105: 200-204.
Direct Link - Colline D.M. and D.M. Stephens, 1991. Identification of an insertion sequence, IS1081, in Mycobacterium bovis. FEMS Microbiol. Lett., 83: 11-16.
Direct Link - De Lassence, A., D. Lecossier and C. Pierre, 1992. Detection of mycobacterial DNA in pleural fluid from patients with tuberculous pleurisy by means of the polymerase chain reaction: Comparison of two protocols. Thorax, 47: 265-269.
Direct Link - DeWit, D., G. Maartens and L. Steyn, 1992. A comparative study of the polymerase chain reaction and conventional procedures for the diagnosis of tuberculous pleural effusion. Tuber. Lung. Dis., 73: 262-267.
Direct Link - Ieven, M. and H. Goossens, 1997. Relevance of nucleic acid amplification techniques for diagnosis of respiratory tract infections in the clinical laboratory. Clin. Microbiol. Rev., 10: 242-256.
Direct Link - Kim, B.J., K.H. Lee, B.N. Park, S.J. Kim, G.H. Bai and Y.H. Kook, 2001. Differentiation of Mycobacterial species by PCR-restriction analysis of DNA (342 Base Pairs) of the RNA polymerase gene (rpoB). J. Clin. Mirobiol., 39: 2102-2109.
Direct Link - Kolk, A.H., A.R. Schuitema, S. Kuijper, J.V. Leeuwen, P.W. Hermans, J.D. Van Embden and R.A. Hartskeerl, 1992. Detection of Mycobacterium tuberculosis in clinical samples by using polymerase chain reaction and a nonradioactive detection system. J. Clin. Microbiol., 30: 2567-2575.
Direct Link - Neimark, H., M. Ali-Baig and S. Carleton, 1996. Direct identification and typing of Mycobacterium tuber-culosis by PCR. J. Clin. Microbiol., 34: 2454-2459.
Direct Link - Parandaman, V., S. Narayanan and P.R. Narayanan, 2000. Utility of polymerase chain reaction using two probes for rapid diagnosis of tubercular pleuritis in comparison to conventional methods. Ind. J. Med. Res., 112: 47-51.
Direct Link - Pietrzak, J., R. Frei, H.P. Senn and C. Moroni, 1994. Comparison of polymerase chain reaction with standard methods in the diagnosis of Mycobacterium tuberculosis infection. Eur. J. Clin. Microbiol. Infect. Dis., 13: 1079-1083.
Direct Link - Querol, J.M., J. Minguez, E.G. Sanchez, M.A. Farga, C. Gimeno and J.G. Lomas, 1995. Rapid diagnosis of pleural tuberculosis by polymerase chain reaction. Am. J. Respir. Crit. Care. Med., 152: 1977-1981.
Direct Link - Ravn, P., M.E. Munk, A.B. Andersen, B. Lundgren and G.D. Lundgren et al., 2005. Prospective evaluation of whole blood test using Mycobacterium tuberculosis-specifice antigens ESAT-6 and CFP-10 for diagnosis of active tuberculosis. Clin. Diag. Lab. Immun., 12: 491-496.
Direct Link - Reechaipichitkul, W., V. Lulitanond, S. Sungkeeree and B. Patjanasoontorn, 2000. Rapid diagnosis of tuberculous pleural effusion using polymerase chain reaction. Southeast Asian J. Trop. Med. Public Health, 31: 509-514.
Direct Link - Scarpellini, P., S. Racca, P. Cinque, F. Delfanti, N. Gianotti, M.R. Terreni, L. Vago and A. Lazzarin, 1995. Nested polymerase chain reaction for diagnosis and monitoring treatment response in AIDS, patients with tuberculous meningitis. AIDS., 9: 895-900.
Direct Link - Sharma, S.K. and A. Banga, 2005. Pleural fluid interferon-gamma and adenosine deaminase levels in tuberculosis pleural effusion: A cost-effectiveness analysis. J. Clin. Lab. Anal., 19: 40-46.
Direct Link - Villegas, M.V., L.A. Labrada and N.G. Saravia, 2000. Evaluation of polymerase chain reaction, adenosine deaminase and interferon-gamma in pleural fluid for the differential diagnosis of pleural tuberculosis. Chest, 118: 1355-1364.
Direct Link - Ibrahim, W.H., W. Ghadban, A. Khinji, R. Yasin, H. Soub, A.L. Al-Khal and A. Bener, 2005. Does pleural tuberculosis disease pattern differ among developed and developing countries. Respir. Med., 99: 1038-1045.
Direct Link