
Aisha Zakaria Hashem Mustafa
Department of Removable Prosthodontics, Faculty of Dentistry, Mansoura University, Egypt
European Journal of Dentistry and Medicine
Year: 2012 | Volume: 4 | Issue: 3 | Page No.: 45-55







ABSTRACT
In rehabilitation of partially edentulous cases with removable prosthesis it is desirable to equalize the retention bilaterally, to allow the removable prosthesis to function accurately without affecting the health of remaining structure. This can be achieved when few remaining teeth is present unilaterally by strategic multiplication of abutment using dental implant. This study describes a treatment approach for oral rehabilitation of patients with remaining teeth on one posterior quarter of the mandibular arch. In mandibular arch one implant was inserted in the canine region to be used in conjunction with natural canine as abutments for removable partial overdenture. For every patient a temporary mandibular RPD were constructed and relined with soft liner to be used during the osseointegration period. After this duplication of implant O-ring ball abutment to be used with metal coping and dowel on the canine then construction of the final RPD and clinical pick up of the O-ring attachments. Marginal bone loss and mobility test were assessed immediately after insertion of the prosthesis and after 3 years of functioning loading of the implant. Regular follow-up visits, through 3 years, revealed that the periodontal and peri-implant conditions were stable; there were no intrusion or mobility problems of the teeth and very minor changes in the bone levels of the natural teeth and implants were measured on radiographs using Corel Draw No.11 software. Duplication of implant O-ring ball abutment to be used with metal coping and dowel on the canine abutment allow even distribution of the load on the implant and canine tooth leading to statistically no significant difference between the bone loss of the implant and tooth or between the mesial and distal sides of the implant or canine tooth.
PDF Abstract XML References Citation
Received: July 18, 2012;
Accepted: August 31, 2012;
Published: November 08, 2012
How to cite this article
Aisha Zakaria Hashem Mustafa, 2012. Duplicating the Implant O-ring Abutment Retainer for Using on Tooth Copy in Mandibular Implant-tooth Partial Overdenture: Radiographic Evaluations. European Journal of Dentistry and Medicine, 4: 45-55.
DOI: 10.3923/ejdm.2012.45.55
URL: https://scialert.net/abstract/?doi=ejdm.2012.45.55
DOI: 10.3923/ejdm.2012.45.55
URL: https://scialert.net/abstract/?doi=ejdm.2012.45.55
INTRODUCTION
In rehabilitation of partially edentulous cases with removable prosthesis, the retention and stability of RPDs is dependent on the state of the alveolar ridge and available teeth to be clasped. Poor RPD retention and stability occurs with highly resorbed ridges and an inadequate number of suitable abutment teeth. RPDs with distal extensions, Kennedy Class I and II, generally have less stability than those of bounded saddle (Brudvik, 1999; Car and Brown, 2011).
Removable Partial Denture (RPD) is a common treatment option available for the restoration of a long-span or distal extension edentulous area where in a fixed partial denture is not indicated. The type of retainer used with the RPD affect the remaining structures (Itoh et al., 2008; Costa et al., 2009). Equalization of the retainer bilaterally can be obtained through tilting the cast laterally to establish reasonable uniformity of retention which is necessary for successful removable partial denture (Car and Brown, 2011).
Clasping anterior teeth creates several problems. First, unacceptable aesthetic results can occur when anterior teeth are clasped and are visible during smiling of the patient. Second, anterior teeth provide inadequate retention for distal extension RPDs (Zitzmann, 2005). Third, anterior teeth can be lost or the clasp can be fractured due to excessive loading (Car and Brown, 2011).
The use of dental implants to aid in support and retention of partial overdentures is one prosthetic option primarily described in the literature in the form of various clinical reports and researches (Keltjens et al., 1993; Giffin, 1996; Uludag and Celik, 2006; Chang et al., 2007; Chikunov et al., 2008; Ohkubo et al., 2008; Grossmann et al., 2009; Vogel, 2011).
The quantity of prosthesis retention and stability depend on attachment type, design, alignment and position (Walton, 1999; Williams et al., 2001). Different methods have been expected for connecting overdentures to underlying implants. Independent connections to each implant abutment or constant bar retainers are the most frequent approaches (Mijiritsky and Karas, 2004; Uludag and Celik, 2006; Schneid and Mattie, 2008).
Root overdenture philosophy postulated a transfer of occlusal forces to the alveolar bone through the periodontal ligament of the retained roots. Proprioceptive feedback from the periodontal ligament was envisaged to act to prevent occlusal overload and consequently avoid residual ridge resorption adjacent to the roots and the rest of the residual ridge because of excessive forces (Crum and Loiselle, 1972; Crum and Rooney, 1978; Renner et al., 1984; Carlsson, 2004). They also provided improved function compared to conventional complete dentures such as improved biting force and chewing efficiency and even phonetics (Rissin et al., 1978; Ghi and McGivney, 1979; Renner et al., 1984). The stability of tooth supported overdentures greater than the non tooth supported overdentures (Murakami et al., 2008).
When the remaining teeth present in unilateral (in one side of the arch) the lifting movement of long saddle of the removable partial denture well be difficult to be counteracted by conventional clasping. A properly positioned implant can permit the fabrication of a retentive and stable RPD that was not possible before and improve the masticatory function (Van Kampen et al., 2004). In addition, the use of an overdenture abutment eliminates the need for an unaesthetic clasping system (Mijiritsky, 2007).
A strategically placed dental implant can establish an improved removable partial denture by significantly reducing the effort arm and improving the fulcrum line position (Mijiritsky, 2007; Car and Brown, 2011).
Implant assisted removable partial denture increase support, retention and stability in order to limit the denture’s movement, leading to reduction of the tension forces generated on the abutment teeth and supporting structure, favoring the maintenance of the supporting structure. Also, it provides patient’s functional and psychological comfort (Shahmiri and Atieh, 2010; De Silva et al., 2011). This well enhances the patient quality of life from both nutritional and social point of view (Spitzl et al., 2012).
This study evaluate radiographically cases treated with Removable Partial Overdentures (RPOD) supported by both implants and natural teeth. Three years after functional loading, the clinical and radiographic changes for implants and natural teeth were reported.
MATERIALS AND METHODS
Ten patients come to clinic of removable prosthodontic, Mansoura University. The patients have remaining mandibular canine and posterior teeth in one side of the arch (Fig. 1a).
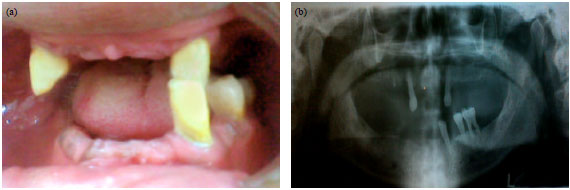 | |
| Fig. 1(a-b): | The case before treatment (a) Intraoral view and (b) Panoramic X-ray |
 | |
| Fig. 2(a-c): | (a) Maxillary zinc-oxide eugenol impression, (b) Plastic dowel in prepared canine and (c) Mandibular pick-up impression (with plastic dowel and implant analog) |
They are free of any systemic disease that affect implant placement. For every patient, a panoramic radiograph were done (Fig. 1b) then strategic implant was inserted opposite to mandibular canine, in canine region for construction of mandibular implant tooth retained partial overdenture.
Step by step technique for every patient:
| Step 1: | After maxillary and mandibular impressions were made, root canal treatments were done in the mandibular canine and preparation was done for dowel. |
| Step 2: | After construction of custom trays, secondary impressions were done and the casts were poured. Then jaw relation was done using record blocks. |
| Step 3: | After try in, the temporary denture were constructed (mandibular acrylic removable partial denture) opposing either maxillary single or overdenture. Then it was inserted intraoral. It was used as surgical stent during implant placement. |
| Step 4: | After one week of insertion of the one piece implant (13 mm height- 3.9 mm width) in right mandibular canine region, the temporary mandibular partial denture were relived in implant region and relined with soft liner to be used in the osseointegration phase of the implant. |
| Step 5: | After 4 months, the final prosthesis was constructed. Secondary maxillary impression were done using zinc oxide eugenol impression material (Fig. 2a) and poured in dental stone. Mandibular pick-up impression of the implant and plastic post was done (Fig. 2b, c). |
| Step 6: | For duplication of the O-ring abutment a rubber base heavy type were used to take impression of abutment analog on the cast. Wire was used to give air way escape during pouring of the wax (Fig. 3a). Then the rubber base sectioned with scalpel passing through the implant ball and reposition the two part to each other and blue inlay wax used to pour this mould (Fig. 3b). |
| Step 7: | After pouring the wax ball abutment, it was fixed to waxed up copy of the tooth then the copy with waxed ball abutment casted (Fig. 4a-c). |
| Step 8: | For constructing record base for jaw relation a wax relief made on two ball abutments. Then a jaw relation recorded. |
| Step 9: | After setting, try-in was done. In the lab, the two ball abutments were blocked out during the denture processing. |
| Step 10: | After correction of occlusal error related to laboratory processing of acrylic resin, widen the opining at the implant and tooth O-ring attachment to allow escape of excess acrylic resin during clinical pick up of O-ring attachment. |
| Step 11: | Spacers were used during clinical pick-up of the O-ring attachment. They were made from tin foil (Fig. 5a). |
| Step 12: | The prosthesis extraoral and intraoral (Fig. 5b, c). |
| Step 13: | Three years radiographic and clinical evaluations (mobility test) were done to monitor the cases. And to measure the alveolar bone level around the mandibular canine and the crestal bone level around the implant. |
| Step 14: | No need for relining was found. |
Method evaluation
Radiographic measurement of the marginal bone level: Corel Draw No.11 software was used to measure the bone level of the canine and implant (Fig. 6).
 | |
| Fig. 3(a-b): | (a) Rubber base impression of ball abutment and (b) The rubber mould after pouring ball abutment that duplicated implant ball |
 | |
| Fig. 4(a-c): | (a) The copy with duplicated ball, (b) O-ring positioned on implant and tooth copy with duplicated ball on the cast and (c) Intraoral view |
 | |
| Fig. 5(a-c): | (a) The O-ring and spacer with prepared denture, (b) The final prosthesis after clinical pick-up of O-ring attachment and (c) Intraoral view |
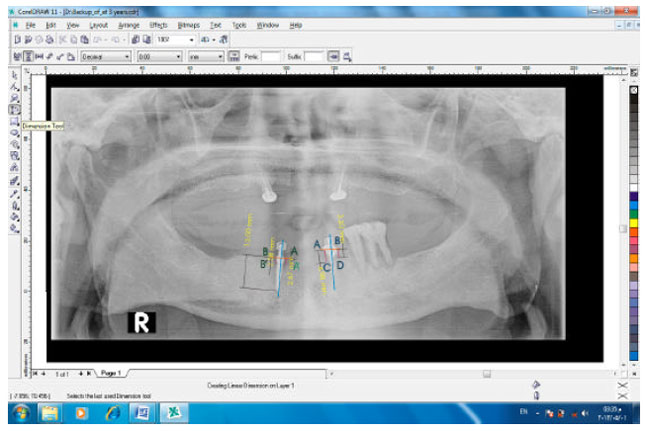 | |
| Fig. 6: | Digital panoramic X-ray after 3 years with CorelDraw 11 software measurements |
To eliminate the radiographic magnification error of panoramic radiograph, the scale of measurement was adjusted according to the actual length of the implant. A standardized digital panoramic radiograph was taken for each patient at denture insertion (functioning loading) and after 3 year to measure the alveolar bone level around the mandibular canine and the crestal bone level around the implant abutments at mesial and distal sides. The mean marginal bone was calculated as follows:
The mean marginal bone level on the implant = (AA'+BB')/2 and (AC+BD)/2 for canine
Mobility index: Implant and canine mobility was assessed manually by the handles of two dental mirrors put on either sides of implant and canine abutments buccolingually as recommended by Gatti et al. (2000).
Statistical analysis: A Student’s t-test was used for the statistical analysis of Tooth alveolar bone change after three years of denture insertion in comparison to the implant crestal bone change. Also it used to compare the mesial with the distal bone change of the implant and tooth. The p-value was set to 0.05 to detect the level of significance. Analysis was performed using SAS software, version 9 (SAS, 2004).
RESULT
Table 1 shows the mean implant crestal bone loss and the mean tooth alveolar bone loss after 3 years of functional loading. It was 0.494±0.110 for the implant and 0.594±0.186 for the tooth. There was no statistically significant difference between the mean bone loss of the implant and tooth in the study period (t =1.46 and p = 0.16). The mean mesial implant crestal bone loss and the mean mesial tooth alveolar bone loss after 3 years of functional loading. It was 0.512±0.149 for the implant and 0.588±0.191 for the tooth. There was no statistically significant difference between the mesial bone loss of the implant and tooth in the study period (t = 0.99 and p = 0.3337). The mean distal implant crestal bone loss and the mean distal tooth alveolar bone loss after 3 years of functional loading. It was 0.476±0.092 for the implant and 0.6±0.206 for the tooth. There was no statistically significant difference between the distal bone loss of the implant and tooth in the study period (t = 1.74 and p = 0.986).
Table 2 shows that there was no statistically significant difference between the mean bone loss of the implant at the mesial and at the distal side (t = 0.65 and p = 0.5231). Also there was no statistically significant difference between the mean bone loss of the tooth at the mesial and at the distal side (t = 0.14 and p = 0.8939).
Mobility index: Mobility index showed zero score during the period of study for both the implant and canine tooth.
| Table 1: | The mean implant crestal bone loss and the mean tooth alveolar bone loss after 3 years of functional loading |
 | |
| Value are significant if p<0.05 | |
| Table 2: | The t-test for comparing the implant bone loss at mesial and distal sides and also tooth bone loss at mesial and distal sides |
 | |
| Value are significant if p<0.05 | |
DISCUSSION
The primary goal of removable prosthodontic is not only to restore what is missing but also to preserve what is remain. Tooth overdenture considered a treatment option to preserve the remaining tissue (Ghi and McGivney, 1979; Spitzl et al., 2012). Traditional overdentures depend on the position of the remaining teeth. When these teeth distributed in a manner that compromise the treatment, implants may be placed in planned, specific sites for overdenture to improve the prosthetic rehabilitation (Misch, 2005).
Limited numbers of implants are used to improve the RPD support, enhance retention and stability, preserve the residual ridge underneath the denture base, reduce the stress applied on the abutment teeth, eliminate the need for unesthetic clasp assemblies and modify unfavorable arch configurations (Zitzmann, 2005; Mijiritsky, 2007). Mijiritsky et al. (2005) point out that: implant-retained RPD, provides distinct biomechanical advantage in improving the fulcrum line position, as well as offering superior retention. Also, Phoenix et al. (2008) added that: implant-assisted RPD increase patient comfort and satisfaction. One of the appropriate positions for the implants in RPD was on the canine positions to provide vertical support and retention.
In this study to offer patients affordable prostheses with better retention, the removable partial denture was retained by a combination of implants and natural teeth by using implant-tooth overdenture. This prosthesis will combine the advantage of implant and the advantage of proprioception of tooth overdenture. To equalize the retention bilaterally an implant inserted in the canine region at the same distance from the midline as the distance to the canine used as overdenture abutment. Also the O-ring abutment of the implant was duplicated for the canine overdenture. Torabinejad and Goodacre (2006) stated that, teeth that have undergone endodontic treatment well be functional over long time as the dental implant. So that, tooth and dental implant was functioning as overdenture abutments for removable partial denture. Also in this study mandibular temporary removable partial denture was constructed and lined with soft liner to be wearied during the Osseo integration period. According to Mutluay and Ruyter (2005) and Chestnut and Gibson (2007). The relived temporary prosthesis, relined with soft liner, to be used during the osseointegration periods, to prevent any trauma to the implant from the denture or hard foods and to minimize direct pressure to the soft tissues.
Due to the difference in resiliency between both, tooth and implant, resilient attachments (O-ring) were used in this study. Srinivasan and Padmanabhan (2008) mentioned that: because of the difference between structures of implants and natural teeth, their mobility also differs. Attempts to incorporate both implants and natural teeth with rigid connection in prostheses should not be made. Intrusion of natural tooth may be caused by reasons other than excessive forces.
To optimize stress distribution and minimize forces to the implant and tooth in overdenture, the resilient ball/O-ring attachment may provide adequate retention while possibly reducing stress on the implant bodies (Kenney and Richards, 1998; Misch, 2005). Also resilient attachments allowed for an increase of the mastication load transiting through denture bearing surface (Daas et al., 2008).
The patient examined regularly to reduce the risk of experiencing caries and periodontal disease of tooth overdenture (Ettinger and Qian, 2004). If the combination of implants and natural teeth is necessary, overloading of implants and intrusion of natural teeth should be monitored carefully (Chang et al., 2007). Three years follow up reveled that there was no intrusion or mobility of the teeth, very minor changes in the bone levels of the natural teeth (0.594±0.186) or implants (0.494±0.110) measured on radiographs. Albrektsson et al. (1986) and Laurell and Lundgren (2011) suggested that: one of the parameters of implant success was the amount of Marginal Bone Loss (MBL). During the first year after abutment connection, 1 mm of MBL is allowed followed by 0.2 mm per year.
This study revealed that there was no statistically significant difference between the mean implant and tooth bone loss in the study period (t = 1.46 and p = 0.16). There was no statistically significant difference between the mesial bone loss of the implant and tooth in the study period (t = 0.99 and p = 0.3337). There was no statistically significant difference between the distal bone loss of the implant and tooth in the study period (t = 1.74 and p = 0.986). This may be attributed to the use of resilient O-ring attachment on the implant and duplication of this attachment to be used on the natural tooth (canine).
O-ring attachment is the most flexible of all the resilient attachment and is therefore of greatest use in situations where implant support is minimal (Brudvik, 1999). The O-ring performs the function of retention and enabling universal free rotation. When the vertical loading is applied to the O-ring attachment, the load can be separated from the implant by the clearance, black plastic ring in its interior and soft tissue. This gives the buffer effect under vertical loading. The non-direct loading produces very low stresses on the implant which can be neglected (Tseng and Jiang, 2004). The O-ring may allow motion in six different directions depending on the resilient depression of the O-rings and the presence of spacer over the post head (Misch, 2005). During the clinical pick up of O-ring attachment on either the implant or the canine a spacer was used to preserve the resiliency of the attachment during functional loading. Misch (2008) stated that: if a superstructure contacts the implant, the range of motion, of implant resilient attachment decrease.
There was no statistically significant difference between the mean bone loss of the implant at the mesial and at the distal side (t = 0.65 and p = 0.5231). Also there was no statistically significant difference between the mean bone loss of the tooth at the mesial and at the distal side (t = 0.14 and p = 0.8939). Phoenix et al. (2008) stated that: in implant assisted RPD when resilient attachment are used occlusal load are transmitted to implant and ridge. This may be one of the causes that prevent the implant overloading in this study.
This study found that in the case of implant- tooth partial overdenture opposed by maxillary single or overdenture on two canine, most supportive forces were born by the mucosa, whereas the implant and tooth of overdenture provided mainly for retention and duplication of the resilient O-ring attachment were done for equalization of retention bilaterally, so that overloading was less likely to occur to either the natural tooth or implant. Patient satisfaction with this prosthesis appears in term of function and aesthetics.
CONCLUSION
The use of strategically placed implant in the canine region to assist a claspless removable partial denture considered a good treatment option for rehabilitation of the patient with unilaterally present few remaining teeth. The benefits gain from this implant was elimination of the lifting movement of the long free end saddle that crosses the midline. This prosthesis will combine the advantage of implant and the advantage of proprioception of tooth overdenture. Duplicating the implant O-ring attachment to be used with metal coping and dowel on the natural tooth (canine) was important to equalize the retention bilateral and allow even distribution of functional load without overloading or compromising both, the implant and natural tooth. Patient satisfaction with implant-tooth removable partial overdenture appears in term of function and aesthetics.
ACKNOWLEDGMENT
I am thankful to Professor. Dr. Ahmed Habib who make the surgery of implant insertion.
REFERENCES
- Albrektsson, T., G. Zarb, P. Worthington and A.R. Eriksson, 1986. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac Implants, 1: 11-25.
PubMed - Chang, L.C., J.C. Wang and C.C. Tasi, 2007. Removable partial denture on osseointegrated implants and natural teeth. Chang Gung Med. J., 30: 274-279.
PubMed - Chikunov, I., P. Doan and F. Vahidi, 2008. Implant-retained partial overdenture with resilient attachments. J. Prosthodont., 17: 141-148.
PubMed - Costa, M.M., M.A. da Silva, S.A. Oliveira, V.L. Gomes, P.M. Carvalho and B.L. Lucas, 2009. Photoelastic study of the support structures of distal-extension removable partial dentures. J. Prosthodont., 18: 589-595.
PubMed - Crum, R.J. and G.E. Rooney, 1978. Alveolar bone loss in overdentures: A five-year study. J. Prosthetic Dentistry, 40: 610-613.
CrossRef - Ettinger, R.L. and F. Qian, 2004. Abutment tooth loss in patients with overdentures. J. Am. Dent. Assoc., 135: 739-746.
PubMed - Gatti, C., W. Haeflieger and M. Chiapasco, 2000. Implant retained mandibular overdenture with immediate loading: A prospective study of ITI implants. Int. J. Oral Maxillofacial Implants, 15: 383-388.
PubMed - Ghi, H. and G.P. McGivney, 1979. Influence of tooth proprioception on speech articulation. J. Prosthetic Dentistry, 42: 609-613.
PubMed - Giffin, K.M., 1996. Solving the distal extension removable partial denture base movement dilemma: A clinical report. J. Prosthetic Dentistry, 76: 347-349.
PubMedDirect Link - Itoh, H., K. Baba, K. Aridome, D. Okada and A. Tokuda et al., 2008. Effect of direct retainer and major connector designs on RPD and abutment tooth movement dynamics. J. Oral Rehabil., 35: 810-815.
CrossRefDirect Link - Keltjens, H.M., A.F. Kayser, R. Hertel and P.G. Battistuzzi, 1993. Distal extension removable partial dentures supported by implants and residual teeth: Considerations and case reports. Int. J. Oral Maxillofacial Implants, 8: 208-213.
PubMedDirect Link - Kenney, R. and M.W. Richards, 1998. Photoelastic stress patterns produced by Implant-retained overdentures. J. Prosthetic Dentistry, 80: 559-564.
PubMedDirect Link - Laurell, L. and D. Lundgren, 2011. Marginal bone level changes at dental implants after 5 years in function: A Meta-analysis. Clin. Implant Dent. Related Res., 13: 19-28.
CrossRef - Mijiritsky, E. and S. Karas, 2004. Removable partial denture design involving teeth and implants as an alternative to unsuccessful fixed implant therapy: A case report. Implant Dent., 13: 218-222.
PubMedDirect Link - Mijiritsky, E., Z. Ormianer, A. Klinger and O. Mardinger, 2005. Use of dental implants to improve unfavorable removable partial denture design. Compend. Contin. Educ. Dent., 26: 744-750.
PubMedDirect Link - Mijiritsky, E., 2007. Implants in conjunction with removable partial dentures: A literature review. Implant. Dent., 16: 146-154.
PubMedDirect Link - Murakami, M., K. Takesako, N. Kawahata, H. Tanaka, Y. Nishi and E. Nagaoka, 2008. Stabilities of maxillary complete overdentures with and without abutment tooth support: Examination by dynamics of atmospheric pressure as an index of denture stability. Prosthodont. Res. Pract., 7: 89-96.
Direct Link - Mutluay, M.M. and I.E. Ruyter, 2005. Direct relining of dentures with soft materials. Tandlaegebladet, 115: 658-659.
Direct Link - Ohkubo, C., M. Kobayashi, Y. Suzuki and T. Hosoi, 2008. Effect of implant support on Distal-extention removable partial dentures: In vivo assessment. Int. J. Oral Maxillofacial Implants, 23: 1095-1101.
PubMedDirect Link - Renner, R.P., B.C. Gomes, M.L. Shakun, P.N. Baer, R.K. Davis and P. Camp, 1984. Four-year longitudinal study of the periodontal health status of overdenture patients. J. Prosthetic Dentistry, 51: 593-598.
CrossRef - Rissin, L., J.E. House, R.S. Manly and K.K. Kapur, 1978. Clinical comparison of masticatory performance and electromyographic activity of patients with complete dentures, overdentures and natural teeth. J. Prosthetic Dentistry, 39: 508-511.
CrossRef - Shahmiri, R.A. and M.A. Atieh, 2010. Mandibular kennedy class I implant‐tooth‐borne removable partial denture: A systematic review. J. Oral Rehabil., 37: 225-234.
CrossRef - De Silva, M.A.B., R.L.X. Consani, G.J.P.L. Oliveira, J.I.L. Reis, L.A. Fontanari and J.M.S.N. Reis, 2011. Association between implants and removable partial dentures: Review of the literature. RSBO, 8: 88-92.
Direct Link - Spitzl, C., P. Proschel, M. Wichmann and S. Heckmann, 2012. Long-term neuromuscular status in overdenture and complete denture patients with severe mandibular atrophy. Int. J. Oral Maxillofacial Implants, 27: 155-161.
PubMed - Srinivasan, M. and T.V. Padmanabhan, 2008. Intrusion in implant-tooth-supported fixed prosthesis: An in vitro photoelastic stress analysis. Indian J. Dent. Res., 19: 6-11.
Direct Link - Torabinejad, M. and C.J. Goodacre, 2006. Endodontic or dental implant therapy: The factors affecting treatment planning. J. Am. Dent. Assoc., 137: 973-977.
Direct Link - Tseng, C.G. and Y.S. Jiang, 2004. Mechanics analysis for implant-soft tissue retained overdenture. J. Chin. Inst. Eng., 27: 405-415.
CrossRef - Uludag, B. and G. Celik, 2006. Fabrication of a maxillary implant-supported removable partial denture: A clinical report. J. Prosthetic Dentistry, 95: 19-21.
CrossRef - Van Kampen, F.M.C., A. van der Bilt, M.S. Cune, F.A. Fontijn-Tekamp and F. Bosman, 2004. Masticatory function with implant-supported overdentures. J. Dental Res., 83: 708-711.
CrossRef - Walton, J.N., 1999. Positioning implants for overdentures: A prototype implant-paralleling device. Technical note. Int. J. Oral Maxillofac Implants, 14: 295-297.
PubMed - Williams, B.H., K.T. Ochiai, S. Hojo, R. Nishimura and A.A. Caputo, 2001. Retention of maxillary implant overdenture bars of different designs. J. Prosthetic Dentistry, 86: 603-607.
Direct Link