
Ahmed Mohamed Mohee Elden Al Bassiouny
Department of Otolaryngology, Faculty of Medicine, Cairo University
Journal of Medical Sciences
Year: 2009 | Volume: 9 | Issue: 3 | Page No.: 118-125







ABSTRACT
In this study, a new surgical technique was designed, with preservation of the palatal dynamics, aiming to nearly abolish the postoperative pain and eliminate snoring recurrence. Patients were selected from Dar Al Shifa Hospital, Kuwait, complaining of snoring and fitting certain preoperative criteria. Thirty two patients were treated with this technique between April 2006 and March 2008, with minimum follow up period of six months. Snoring cured in 22 patients (69%), improved in 7 patients (22%) and failure in 3 (9%) cases. No recurrence of snoring was observed during the 6 months of follow up period. Postoperative pain reduced in both duration and severity. This new surgical technique may be an effective method in reducing postoperative pain and elimination of the possibility of palatal fibrosis and retraction, both medial and posterior and so reducing the incidence of postoperative recurrence of snoring owing to absence of raw surface at the free edge of the soft palate.
PDF Abstract XML References Citation
How to cite this article
Ahmed Mohamed Mohee Elden Al Bassiouny, 2009. Posterior Pillar Flap Palatoplasty: A New Surgical Technique for Treatment of Snoring: Initial Experience. Journal of Medical Sciences, 9: 118-125.
DOI: 10.3923/jms.2009.118.125
URL: https://scialert.net/abstract/?doi=jms.2009.118.125
DOI: 10.3923/jms.2009.118.125
URL: https://scialert.net/abstract/?doi=jms.2009.118.125
INTRODUCTION
Snoring is a common social problem that may occur alone or as a sign of a more serious condition; obstructive sleep apnea.
Many procedures were developed during the past 2 decades, but which procedure, if any, is preferable is controversial. No single procedure has been proven to have the ideals that justify its sole use over other (Quinn et al., 1995).
Ikematsu (1964) described uvulopalatophar-yngoplasty (UPPP), the first surgical treatment for snoring.
Fujita (1984) introduced the procedure, with slight modifications. The new procedure quickly became the gold standard.
The limitations of UPPP created a demand for a more effective, safe and comfortable alternative. Kamami (1990) introduced what initially called O2 laser vaporization of the palatopharynx. Coleman introduced the procedure in 1992, but by then it had been modified and was called the laser-assisted uvulopalatoplasty (LAUP).
Concern over the morbidity caused by UPPP and LAUP led to a search for a technique that is simple and minimally invasive and that does not interfere with normal velopharyngeal function. Ellis et al. (1993) used a mechanical model to demonstrate that stiffening the soft palate, rather than shortening it, can reduce the palatal flutter of snoring.
Another development was the Cautery-Assisted Palatal Stiffening Operation (CAPSO), in which the surgeon uses Electrocautary to remove a longitudinal strip of mucosa along the soft palate and the anterior uvula (Mair and Day, 1996). The uvulopalatal flap, is a recently described by Powell et al. (1996) and offered several theoretical advantages over traditional UPPP.
Recently, Powell et al. (1998) used radiofrequency energy in the soft palate, to establish a new procedure called radiofrequency ablation (RFA) or Somnoplasty.
Dickson and Blokmanis (1987) has been described the ideal excision point in surgery for redundant soft palate and uvula, 4 to 5 mm below the palatal dimple, which delineates the lower end of the levator palati muscles. This part of the soft palate is not necessary for normal phonation or velopharyngeal closure. It is, however, the main source of vibration seen on simulated snoring.
This study try to overcome the disadvantages of other surgical techniques regarding postoperative pain and minimizing the interference with palatal dynamics with lesser degrees of recurrence of snoring.
MATERIALS AND METHODS
Between April 2006 and March 2008, 32 patients were evaluated in the Dar al Shifa Hospital, Kuwait, complaining primarily from loud snoring.
All patients completed a preoperative questionnaire and underwent complete examination.
A complete history, including lifestyle risk factors; tobacco, alcohol consumption, snoring details, possibility of OSA symptoms and presence of any medical problems.
Patients were completing a questionnaire about there snoring:
| • | My bed partner has complained about my snoring? |
| • | I only snore on my back? |
| • | I snore no matter whatever position I sleep in? |
| • | My snoring disturbs people in the next room? |
| • | My snoring has gotten worse over the last few years? |
| • | My bed partner tell me that I sometimes stop breathing between snores? |
| • | Have you often feel tired after your sleep? |
| • | I snore at night and I am sleepy during the day? |
All patients complete the Epworth Sleepiness Scale to determine the level of daytime sleepiness.
A body mass index was measured in all cases.
A full medical and otorhinolaryngologic examination was performed, with particular attention on: obstructing nasal conditions, enlargement of nasopharyngeal lymphoid tissue, size of the tonsil, configuration of the soft palate and the size of the base of tongue.
Flexible fibroptic nasopharyngoscopy was done to:
| • | Determine any fixed blockages in the upper airway such as a deviated septum or nasal polyps |
| • | Do simple manoeuvres: Muller's manoeuvre to detect the site and degree of airway collapse and Jaw thrust (mandibular advancement); to detect the role of base of tongue in airway obstruction |
Polysomnogram was performed to role out the possibility of OSA in suspected cases.
Patients were included in this study when they met with the following criteria:
| • | Loud disruptive snoring |
| • | Redundant vibrating soft palate and uvula with webbed posterior tonsillar pillars |
| • | Non obstructing nasal condition |
| • | Non obstructing tonsils |
| • | Absence or mild OSA with apnea index less than 15 |
Procedure: The same surgeon performed all operations, which was done in the otolaryngology department of the Dar Al Shifa hospital, Kuwait.
Anesthesia
| • | General anesthesia with patients in tonsillectomy position was used |
| • | Local anesthesia: the space between the 2 mucosal layers of the posterior pillars, the area of the soft palate above the palatal arch and at the junction of the soft palate with the uvula is injected lidocaine 2% with epinephrine 1:100,000 using dental syringe |
Steps
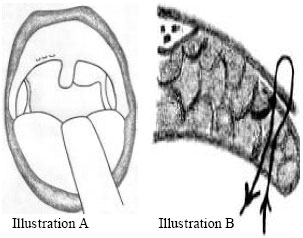
| • | Using the fine tip surgical scissor, the oropharyngeal mucosal layer of the webbed posterior pillar is dissected from the other mucosal layer starting at the junction with the uvula going down towards the lower margin of the posterior pillar (Fig. 1A, B, 2A, B and 7) |
| • | The oropharyngeal mucosal layer of the posterior pillar is removed up the junction of the pillar with the soft palate (Fig. 3A, B) |
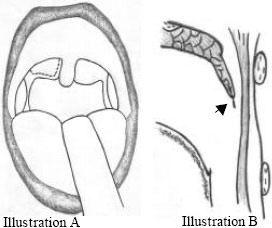 | |
| Fig. 1: | Line of incision of posterior pillar, (A) coronal view and (B) sagittal |
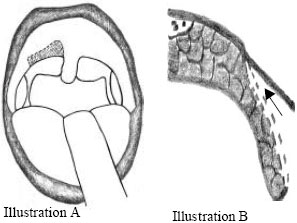 | |
| Fig. 2: | (A, B) Dissection of both mucosal surfaces of the posterior pillar done. Arrow denotes the direction of dissection for the submucosal tunnel |
| • | A submucosal dissection is created in the under surface of the palatal mucosa above the whole width of the posterior pillar to creates submucosal tunnel (Fig. 4A, B) |
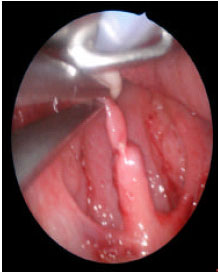
| • | Part of the nasopharyngeal mucosal layer of the posterior pillar is removed and the rest of the pillar mucosa, about 4-5 mm is turned to enter in the submucosal tunnel that created before, (Fig. 4) and sutures taken using absorbable vicryl with straight needle, (pillar mucosa is sutured to the above oral soft palatal mucosa) (Fig. 5A, B, 8, 9 and 10). Before turning the nasopharyngeal mucosal layer of the posterior pillar areas of submucosal diathermy done on the nasopharyngeal surface of the pillar to create raw areas on this surface to allow healing with the inner surface of palatal mucosa |
| • | Lastly, the uvula is shortened (Fig. 6, 9, 10) |
| • | The same steps are done on the other side |
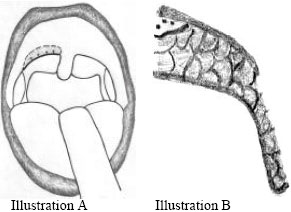 | |
| Fig. 3: | (A, B) Creation of the submucosal palatal tunnel, dotted area and removal of the oropharyngeal layer of the webbing |
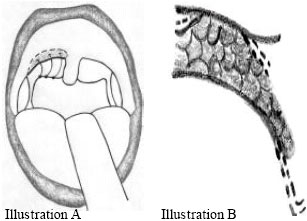 | |
| Fig. 4: | (A, B) The nasopharyngeal layer of webbing will be shortened and rolled up to the submucosal palatal tunnel |
 | |
| Fig. 5: | (A, B) Suture; the nasopharyngeal layer sutured to the oropharyngeal layer 5 mm from the free edge of the soft palate. Knob facing the nasopharynx |
 | |
| Fig. 6: | Shortening of the uvula |
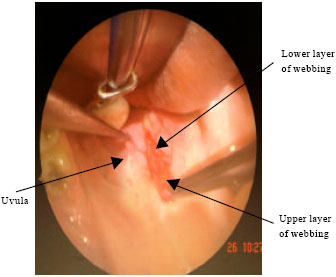 | |
| Fig. 7: | Dissection of both layers of posterior pillar |
 | |
| Fig. 8: | Right side webbing done |
 | |
| Fig. 9: | Both sides done. Uvula marked at site of cutting |
 | |
| Fig. 10: | Suture, intraoperative view |
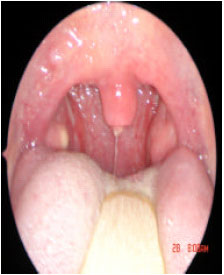
Figure 11-14 show postoperative follow up and Fig. 15 shows the preoperative palate.
Postoperative medication and instructions
| • | Pain killers, paracetamol 500 mg |
| • | Prophylactic systemic antibiotic |
| • | Local antiseptic mouth gargle |
| • | Patients were instructed to eat semisolids and avoid completely the solid foods at least for 5-7 days |
Postoperative follow up
| • | Patients were followed up regularly postoperatively at the end of weeks 1 and 2 and months 1 and 3 after surgery |
| • | Patients follow up was concerned with the following items: |
 | |
| Fig. 11: | One week postoperative |
 | |
| Fig. 12: | Two week postoperative |
 | |
| Fig. 13: | Three week postoperative |
 | |
| Fig. 14: | One month postoperative |
 | |
| Fig. 15: | Preoperative palate |
| • | Stability of the sutures and the reflected mucosal layer |
| • | Pain |
| • | Duration |
| • | Severity: 0 to 10 visual analogue scale was used |
| • | Improvement of snoring as regards loudness and frequency |
Improvement of snoring was classified into three categories as:
| • | Cured: Complete elimination or significant reduction by more than 70% |
| • | Improved: Reduction to an acceptable level of 30 to 70% |
| • | Failure: No change or reduction less than 30% |
The questionnaire asked patients to indicate their level of snoring before and after their surgery as perceived by their partner, family and colleagues on a visual analog scale.
| • | Occurrence of tight palate, with loss of soft palatal shape and configuration |
RESULTS
From April 2006 and March 2008, 32 snorers have been treated with this new technique. They were 26 (81%) male and 6 (19%) females. The mean age was 43.3 (age range between 32 and 56 years). Mean (range) weight (kg) 87.5 The mean body mass index was 28.2.
Table 1, show Patient data, age and weight.
Snoring was cured or improved as regards both loudness and frequency (Table 2). Twenty two patients (69%) was cured 7 patients (22%) were improved and failure occurred in 3 (9%) cases.
Snoring visual analog score was improved from 8.9±0.9 to 2.3±0.4 (p<0.001).
No need for a second operation in any of the patients. No change of palatal configuration or retraction was observed during the follow up period.
The use of this new technique resulted in improvement of outcome in snoring surgery with reduction of number of revision palatoplasty operations.
Postoperative pain: All patients were given a prescription for pain killer in the form of paracetamol 500 mg.
| Table 1: | Patient data: age and weight |
 | |
| Table 2: | Snoring improvement and postoperative pain |
 | |
| Table 3: | Postoperative complications |
 | |
Most of patients feel only mild sorethroat and need only to take analgesia on occasion in the 1st 2-3 days postoperatively (Pain scor after 2 days was 6.1, pain scor after 1 weeks 2.4) (Table 2).
Postoperative pain with this technique become less considered problem in comparison to other palatoplasty operations.
Side effects and complications: Apart from Postoperative pain, there were less common complications than other palatoplasty techniques.
Excessive postnasal discharge occurred in 9 cases (28%) due to shortening of the uvula. the condition starts to improve in most of cases between 2-3 weeks postoperatively. Only one case lasting 4 weeks to starts to improve.
Temporary velopharyngeal insufficiency (VPI) occurred in 3 cases and starts to improve at the end of the 1st week. No reported cases of permanent VPI.
Drinking problems, sensation of dryness and food sticking was observed in some cases (Table 3).
No serious intraoperative or immediate postoperative complications were reported.
The immediate and delayed complications of palatoplasty operations have been reduced greatly with this technique that preserve the anatomical roles of the soft palate and avoid the occurrence of undesired palatal fibrosis which considered one of the major factors for recurrence of snoring.
DISCUSSION
Habitual snoring is a socially disabling problem for a large number of people and is a frequent complaint presented to otolaryngologists.
Snoring can be much more than a simple nuisance and may signal a more significant Sleep-Disordered Breathing (SDB) problem). airway collapse can occur anywhere from the nasal valves to the hypopharynx. Partial airway collapse and tissue vibration at the level of the palate is the usual cause of the snoring component of SDB. Treatment of the palate is usually very successful in alleviating obstruction at this level (Friberg et al., 1995).
Uvulopalatophayngoplasty (UPPP) has been the mainstay of surgical treatment of habitual snorers. Although, successful in sector more than three quarters of patients, it is not without well-described risks and complications (Croft and Golding-Wood, 1990). In recent years, a number of alternative palatal procedures have been reported for office-based treatment of the palate. These are generally offered for snoring, but some also may have application for more significant forms of SDB. They include laser-assisted uvulopalatoplasty (LAUP), the Cautery-Assisted Palatal Stiffening Operation (CAPSO), radiofrequency volumetric tissue reduction (RFVTR) of the palate and others (Mair and Littlefield, 1999).
All of these treatments attempt to reduce the vibratory component of the soft palate and uvula to reduce snoring.
In this study, snoring elimination also is obtained by removal of the vibrating portion of the soft palate with less degree of intra operative and postoperative complications of some of snoring surgery techniques, less interference with palatal dynamics and lesser degrees of recurrence of snoring.
The carbon dioxide laser or cautery is used to cut or vaporize palatal tissue, leaving a raw surface that subsequently undergoes scaring. This raw surface produced after LAUP, leads to circumferential scarring, posteromedial traction of the posterior pillars and medial traction of the lateral wall with subsequent diminution in the nasopharyngeal air space (Finkelstein et al., 1993).
In this study, circumferential scarring, posteromedial traction of the posterior pillars and medial traction of the lateral wall is prevented by covering of the raw area at the free edge of soft palate with the posterior surface of the posterior pillar, thus interrupting the line of fibroses and leaving a healthy mucosa of the edge of the soft palate. By this technique, preservation of the transverse diameter of the soft palate and the circumference of the nasopharynx is obtained. Therefore, recurrence of snoring is reduced or eliminated.
In this new technique, the stability of the reflected mucosa of the posterior pillar and therefore the success of the technique is maintained by:
| • | The good size and width (covering the whole distance from the side of the uvula till the upper pole of the tonsil) of the reflected mucosa and so covering the whole raw area at the free border of the soft palate |
| • | Sutures |
| • | Taking the sutures within the substance of the reflected mucosa and the between the 2 layers of the soft palate away from the edges and not edge to edge |
| • | Making the knob of the sutures on the nasopharyngeal surface of the soft palate and not on the oral aspect, so become away from contact with food decreasing the possibility of suture disruption |
| • | Site of sutures: Taken 4-5 mm above the free edge of the soft palate and so site of suture healing will be away from the edge and so preventing any contracture of free edge of soft palate |
| • | Postoperative edema and infection palate at the site of surgery was reduced by gentle tissue manipulations with minimal use of bipolar cautery |
In this way, good stability of the reflected mucosa is obtained and so no possibility of occurrence of fibrosis preventing circumferential scarring and maintaining the circumference of the nasopharynx.
Also, covering of the raw area and minimal muscle cutting reduces greatly the postoperative pain.
Postoperative pain is one of the most obvious problems that related to LAUP or cautery assisted palatoplasty or even some surgical palatal techniques and one of the main factors because of if which most patients refuse any further interference to reduce snoring more. Wareing and Mitchell (1996) in their study to treat snoring with CO2, showed that the pain in the postoperative period can not be understated and would appear to be best described as the worst sore throat that you have ever had and careful preoperative counseling in this respect is mandatory. They suggested that cutting of muscle with the laser is the causative factor.
In this study, the problem of postoperative pain is reduced in severity and duration, because of avoidance of the possible factors that contribute to this postoperative pain, mainly, the exposed raw area is covered by reflection of the mucosa of the posterior pillar and muscle cutting was only in the limited areas of the palate.
CONCLUSION
Snoring surgery has undergone extensive changes. A number of techniques have been described to improve patient selection for snoring surgeries, but the reliability of each of these procedures has been brought into question.
In this study, this new surgical technique can be an alternative to overcome the disadvantages of other surgical techniques regarding reduction of postoperative pain and minimizing snoring recurrence, owing to absence of palatal raw surface, with less interference with palatal dynamics.
REFERENCES
- Dickson, R.I. and A. Blokmanis, 1987. Treatment of obstructive sleep apnea by uvulopalatopharyngoplasty. Laryngoscope, 97: 1054-1059.
Direct Link