
Mariam A.M. Al-Beiti
Obstetrics and Gynecology Hospital at Fudan University, Shanghai 200011, China
Xin Lu
Obstetrics and Gynecology Hospital at Fudan University, Shanghai 200011, China
Research Journal of Obstetrics and Gynecology
Year: 2008 | Volume: 1 | Issue: 1 | Page No.: 6-8







ABSTRACT
The aim of this study was to evaluate the management of a large, asymptomatic uterine fibroid diagnosed during pregnancy. A 31-year-old female patient, primigravida, 23 weeks 4 days gestation. Ultrasound evaluation revealed fetal anomaly and multiple uterine fibroids. Termination of pregnancy by hysterotomy was decided. In the case of termination of pregnancy associated with large cervical myoma, which causes obstruction of the birth canal, a hysterotomy or cesarean section should be performed.
PDF Abstract XML References Citation
How to cite this article
Mariam A.M. Al-Beiti and Xin Lu, 2008. Termination of Pregnancy in the Second Trimester by Hysterotomy in View of Huge Cervical Fibroid. Research Journal of Obstetrics and Gynecology, 1: 6-8.
DOI: 10.3923/rjog.2008.6.8
URL: https://scialert.net/abstract/?doi=rjog.2008.6.8
DOI: 10.3923/rjog.2008.6.8
URL: https://scialert.net/abstract/?doi=rjog.2008.6.8
INTRODUCTION
Uterine leiomyomas are benign neoplasms which are very prevalent in gynaecology practice, affecting mainly women in reproductive age (Berek, 2002). The prevalence of leiomyoma during pregnancy is reported as 2% (Lolis et al., 2003). Cervical fibroids are relatively rare, usually single. They cause distortion and elongation of the cervical canal and displace the body of the uterus upwards.
Cervical myoma involved with excessive growth, may cause pressure symptoms (Jeffcoate, 2001). During pregnancy, cervical fibroids can grow and sometimes will occlude the birth canal, requiring a cesarean section.
In the present case because of fetal anomaly and the need of termination of pregnancy, which was complicated by a large cervical fibroid, the patient underwent hysterotomy and myomas were left in situ (because of the increased risk of bleeding and postoperative morbidity during myomectomy), with no intra or postoperative complication.
CASE REPORT
A 31-year-old primigravida, presented with 6 months amenorrhea, abdominal swelling with ultrasonographic diagnosis of fetal anomaly and multiple uterine fibroids.
In her gynaecological history, the patient menarche at 13 years old, regular cycle 5/30-35 days, average amount. No other relevant history such as urinary retention or constipation.
Physical Examination: General, cardiovascular and respiratory systemic examinations revealed no abnormalities.
Abdominal Examination: Distended abdomen, right lower abdominal mass about 13x13 cm, regular, firm, non tender with restricted mobility was felt. Fundal height 25 cm, abdominal circumference 88 cm.
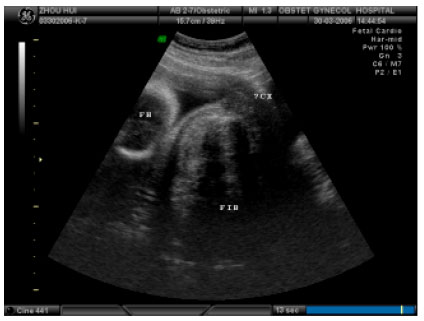 | |
| Fig. 1: | A transabdominal ultrasonogram demonstrating a huge cervical leiomyoma in 31-year old pregnant woman |
Ultrasound Examination Revealed the Presence of Fetal Anomaly: Septum pellucidum not seen, connected anterior horn of lateral ventricles of brain, dilated of the posterior horn of lateral ventricles. Right lower anterior uterine wall prominent, hypoechoic area, measuring 13x13x11 cm, right lower anterior uterine wall hypoechoic lesion with regular outline, measuring 4.1x3.8x5.3 cm, anterior intramural hypoechoic area with regular outline, measuring 4.3x3.5x 3.5 cm and right lower posterior uterine wall hypoechoic lesion measuring 9x9x8.4 cm (Fig. 1).
Ultrasound Suggested
| • | Septum pellucidum deficiency, dilated ventricular system, maldevelopment of optic nerve of septum pellucidum, sign of fore encephalic changes |
| • | Multiple uterine fibroids, one of them obstructs the birth canal, cervical fibroid was suspected |
The situation was discussed with the patient in detail. The decision to terminate the pregnancy was taken. A hysterotomy was proposed and myomectomy was avoided, due to the size and position of the fibroid.
At hysterotomy, uterus was about 28 weeks, left uterine wall, posterior lower uterine wall and cervical fibroids measuring 13, 6, 3 and 9 cm in diameter, respectively.
Termination of pregnancy by hysterotomy for breech presentation was performed and myomectomy of a single fibroid about 3x2x2 cm in the anterior uterine wall was done, others were left in situ due to the increased vascularization of the uterus during pregnancy and women are at increased frequency of post partum haemorrhage and postoperative morbidity during myomectomy. There were no complications during and in the postoperative period. The histopathology report stated uterine smooth muscle fibroid with red degeneration. Chromosome investigation was normal. The patient refused autopsy of the fetus.
DISCUSSION
Rapid growth of cervical fibroids is uncommon. In pregnancy, fibromyomas may increase in size (Cunningham, 1997; Glavind et al., 1990). This will lead to greater surgical difficulty and myoma may be impacted in the pelvis, causing obstruction of the birth canal. During pregnancy, uterine leiomyoma are usually asymptomatic but may be occasionally complicated by red degeneration and an increased frequency of obstructed labour, cesarean section and post partum haemorrhage (Lolis et al., 2003; Brown et al., 1999). Because of the increased vascularization of the uterus during pregnancy, women are at increased risk of bleeding and postoperative morbidity during myomectomy (Brown et al., 1999; Ezechi et al., 2003; Ehigiegba and Evbuomwan, 1998; Depp, 2002; Cunningham et al., 2000). The management of uterine leiomyoma during pregnancy is largely expectant and its surgical removal is generally delayed until after delivery (Ezechi et al., 2003; Ehigiegba and Evbuomwan, 1998).
In case of normal fetus, pregnant women with myoma should undergo frequent ultrasound evaluation during pregnancy in order to monitor both fetal growth and myoma size (Lolis et al., 2003). Most myomas remain asymptomatic during pregnancy and routine ultrasonography performed at this time improves the detection of these lesions and the evaluation of any possible complications (Lolis et al., 2003).
Controversy persists among reports of myomectomy being performed during pregnancy (Lolis et al., 2003); with some case series having reported the safety of antepartum myomectomy in carefully selected patients (Lolis et al., 2003; Burton et al., 1989).
The present case is primigravida, 23 weeks 4 days gestation with documented fetal anomaly, so the decision of termination of pregnancy becomes inevitable. The presence of huge cervical fibroid made the trial of vaginal delivery seem to be quite difficult because of the birth canal obstruction. Therefore, a hysterotomy was preferred in this case and the operation was smooth without any suspected complication such as post partum haemorrhage. Myomectomy was not performed due to the size and position of the fibroid and the increased risk of bleeding and postoperative morbidity during myomectomy.
REFERENCES
- Brown, D., H.M. Fletcher, M.O. Myrie and M. Reid, 1999. Caesarean myomectomy: A safe procedure. A retrospective case controlled study. Obstet. Gynecol., 19: 139-141.
CrossRefDirect Link - Burton, C.A., D.A. Grimes and C.M. March, 1989. Surgical management of leiomyomata during pregnancy. Obstet. Gynecol., 74: 707-709.
PubMedDirect Link - Ezechi, O.C., B.K.E. Kalu, P.E. Okeke and C.O. Nwokoro, 2003. Inevitable cesarean myomectomy: A case report. Trop. J. Obstet. Gynaecol., 20: 159-160.
Direct Link - Lolis, D.F., S.N. Kalantaridou, G. Makrydimas, A. Sotiriadis, I. Navrozoglu, K. Zikopoulos and E.A. Paraskevaidis, 2003. Successful myomectomy during pregnancy. Hum. Reprod., 18: 1699-1702.
Direct Link