
A. S. Shirazi
Department of Radiology, Golestan Hospital, Ahvaz Jundishapur University of Medical Sciences, Ahwaz, Iran
M. Sametzadeh
Department of Radiology, Golestan Hospital, Ahvaz Jundishapur University of Medical Sciences, Ahwaz, Iran
R. Kamankesh
Department of Radiology, Golestan Hospital, Ahvaz Jundishapur University of Medical Sciences, Ahwaz, Iran
F. Rahim
Physiology Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahwaz, Iran
Pakistan Journal of Biological Sciences
Year: 2010 | Volume: 13 | Issue: 4 | Page No.: 190-193







ABSTRACT
This study was conducted to assess the efficacy of ultrasound in the diagnosis of acute appendicitis in clinically suspected cases of acute appendicitis. A total of 110 patients clinically suspected to have acute appendicitis admitted to the surgery departments of Golestan and Imam Khomeini hospitals, from March 2006 to 2007. Abdomino-pelvic ultrasonography with focus on RLQ ultrasonographying the graded compression technique was done. Positive ultrasonography was defined as at least one of the criteria of puylaert. The sonographic data were prospectively correlated with clinical, operative and pathological findings. Graded compression ultrasonography results were analyzed and remarked 92.7% sensitivity, 94.5% specificity, 93% accuracy, 94.4% positive predictive value and 92.5% negative predictive value. Ultrasonography is an accurate, safe and reliable method in the diagnosis of suspected cases of acute appendicitis that can help to minimize negative appendectomies and perforation rates.
PDF Abstract XML References Citation
How to cite this article
A. S. Shirazi, M. Sametzadeh, R. Kamankesh and F. Rahim, 2010. Accuracy of Sonography in Diagnosis of Acute Appendicitis Running. Pakistan Journal of Biological Sciences, 13: 190-193.
DOI: 10.3923/pjbs.2010.190.193
URL: https://scialert.net/abstract/?doi=pjbs.2010.190.193
DOI: 10.3923/pjbs.2010.190.193
URL: https://scialert.net/abstract/?doi=pjbs.2010.190.193
INTRODUCTION
Appendicitis is one of the most common causes of acute abdomen requiring surgical intervention. The preoperative clinical diagnoses are straightforward in 70-80% of cases with an overall negative appendectomy rate of 20-25% (Yu et al., 2005; Lee et al., 2005; Birnbaum and Wilson, 2000; Paulson et al., 2003). Accurate and prompt diagnoses followed by early surgery are essential to minimize morbidity. Because of wide spectrum of clinical presentation and a constant effort to reduce negative appendectomy rate, delay in diagnosis is not uncommon leading to unacceptable rise in perforation rate and significantly increased morbidity and mortality. Females of childbearing age have the highest negative appendectomy rate of 35-45%, because of gynecological conditions simulating appendicitis (Paulson et al., 2003; Yamauchi et al., 2008). In recent years, ultrasonography has been widely performed during the examination of patients with clinically suspected acute appendicitis because of its safety and diagnostic accuracy (Assefa et al., 2006; Morin, 2008). Abdominal ultrasonography was first performed in 1981 to demonstrate an inflamed appendix (Rompel et al., 2006). Since then, many studies have found promising value in abdominal ultrasonography for the diagnosis of acute appendicitis (Yu et al., 2005; Lee, 2003; Zielke et al., 2001). These studies show a sensitivity of 75 to 98% and accuracy of 76 to 96% (Yu et al., 2005; Assefa et al., 2006; Lee, 2003). Thus, negative appendectomy rate can be significantly reduced by ultrasonography along with clinical evaluation (Styrated et al., 2000; Fujii et al., 2000).
The aim of this study was to assess the efficacy of graded compression ultrasonography of the abdomen and pelvis in patients clinically suspected to have acute appendicitis. Many studies have been focused on imaging findings of acute appendicitis but since, the race, diet and normal flora of GI tract in each area can influence on the variety of the human anatomy as well as presentation of appendicitis, with this reason we duplicated the study.
MATERIALS AND METHODS
Patients population and evaluation: A total of 110 patients with acute abdominal pain and tenderness of RLQ, clinically suspected to have acute appendicitis admitted to the department of surgery of Golestan and Imam Khomeini hospitals from March 2007 to March 2009. They referred to ultrasound department and ultrasonography was performed using 3.5 MHz convex and 7.5 MHz linear transducers. After taking a detailed history, performing a complete physical examination and taking blood sample for complete blood count, a plain abdominal radiography examination was performed.
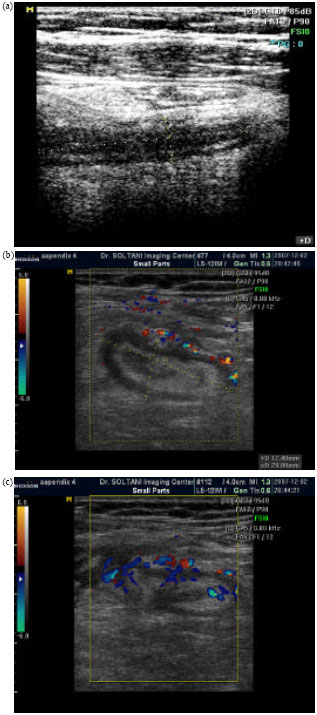 | |
| Fig. 1: | (a) Transverse section of appendicitis, (b, c) longitudinal image of inflamed appendix |
The results were judged positive if the examination met at least one of the criteria of puylaert: (1) non-compressible, swollen appendix with a diameter greater than 7 mm and a wall thickness greater than 3 mm, (2) lack of normal wall layer, (3) appendicolith (4) increase and hyperechogenicity of periappendiceal fat, (5) appendiceal abscess and (6) periappendiceal fluid collection (Fig. 1a-c).
Ultrasonography: We systematically performed a general examination of the entire abdomen by 3.5 MHz convex transducer and a graded compression ultrasonography of right lower quadrant and point of maximum tenderness by a 7.5 MHz transducer. Para-sagittal, transverse and oblique images were obtained until the entire region of interest was scanned. Sonographic findings of each patient were recorded. Preoperative and histopathological findings of all subjects who underwent appendectomy were also recorded separately. The investigators analyzing the data were unaware of the final diagnosis and outcome in each case.
Statistical analysis: Statistical analysis was performed with SPSS software (v.12.0; SPSS Inc., Chicago, IL, USA). Results were expressed as Mean±SD. A probability value of less than 0.05 was considered to be statistically significant. Sensitivity and specificity were calculated according to standard formulas, namely:
and
where, TP is true positives, FN is false negatives, TN is true negatives and FP is false-positives. The predictive values (PV), whether positive (+) or negative (–), were similarly calculated, with +PV being (TP) / (TP + FP) and -PV being (TN) / (TN + FN).
RESULTS
A total of 110 clinically suspected cases of acute appendicitis were examined by sonography. There were 46 (41.82%) male and 64 (58.18%) female patients with mean age of 28.9 years (range 4 to 70 years). Diagnostic results of graded compression ultrasonography are shown in Table 1. There were 56 patients with negative ultrasonography. Of these, four were falsely negative, all four patients had surgery because of persistent pain and acute appendicitis was confirmed on pathological examination. The diagnoses for the 52 patients who tested true negative on diagnostic ultrasonography are shown in Table 1. The sensitivity, specificity, accuracy, positive predictive value and negative predictive value were 92.7, 94.5, 93, 94.4 and 92.5%, respectively. There were 54 patients who had positive ultrasonography studies and subsequently had surgery. Of these, 51 patients had pathological confirmation of acute appendicitis and three were falsely positive. Of the latter, one had a ruptured ovarian cyst and the other two had normal appendix without any problem (Table 2).
| Table 1: | Diagnostic indices of sonography for all study patients |
 | |
| Study group (n = 110) | |
| Table 2: | Ultrasonography findings in sonographically positive patients |
 | |
| The patients had either a single or a combination of the above findings | |
| Table 3: | Diameter of appendix (mm) in cases of appendiceal swelling |
 | |
| Table 4: | Diagnoses of patients who tested true negative on ultrasonography for acute appendicitis |
 | |
Ultrasonography findings of the 54 sonographically positive patients are shown in Table 3. Of these, the swollen appendix with the mean diameter of 8 mm was the most imaging finding (Table 4).
DISCUSSION
Acute appendicitis remains the most common surgical emergency with a life-time occurrence of 7% (Friday, 2006). The key to successful management of acute appendicitis depends on prompt diagnosis and early surgical intervention. The clinical diagnosis of acute appendicitis is not always straightforward and negative appendectomy rate of 20-25% is not uncommon. There is an inverse relationship between negative appendectomy rate and perforation rate. So, the challenge for a surgical specialist is how to balance between efforts to reduce negative appendectomy rate without increasing the perforation rate. Imaging can play a great role in making an early diagnosis of appendicitis and also suggest alternative diagnosis thereby reducing both negative appendectomy rate as well as perforation rate.
Graded compression ultrasonography as popularized by puylaert is a readily available, noninvasive, highly accurate mean of diagnosing appendicitis and a variety of relevant disease (Chan et al., 2005). Prospective studies have shown the overall accuracy of ultrasonography in diagnosing acute appendicitis ranges between 87-98% (specificity 89-99%, sensitivity 86-97%), respectively (Fujii et al., 2000; Chan et al., 2005; Khanal et al., 2008; Himeno et al., 2003; Wiersma et al., 2009). However, in pregnant women and children, the error rate is reported to be much higher, 35-45% but, in this series of 110 patients included 7 children under age 10 years and 3 pregnant women, sonographic diagnoses was correct (Wiersma et al., 2009; Basaran and Basaran, 2009). Of the 7 children, 4 had negative ultrasonography findings and 3 were positive (two cases with swollen appendix measuring 7 and 7.4 mm in total diameter and one with appendiceal abscess). Our data (sensitivity 92.7%, specificity 94.5%, accuracy 93%, positive predictive value 94.4% and negative predictive value 92.5%) confirmed the value of ultrasonography in the diagnosis of acute appendicitis and has produced comparable results to the current literature.
CONCLUSION
Ultrasonography is an accurate, safe and reliable method in the diagnosis of suspected cases of acute appendicitis that can help to minimize negative appendectomy and perforation rates.
REFERENCES
- Assefa, G., S. Meseret and Y. Nigussie, 2006. The role of ultrasound in diagnosing acute appendicictis. Ethiop. Med. J., 44: 67-74.
PubMed - Basaran, A. and M. Basaran, 2009. Diagnosis of acute appendicitis during pregnancy: A systematic review. Obstet. Gynecol. Surv., 64: 481-488.
PubMed - Birnbaum, B.A. and S.R. Wilson, 2000. Appendicitis at the millennium. Radiology, 215: 337-348.
PubMed - Chan, I., S. Bicknell and M. Graham, 2005. Utility and diagnostic accuracy of sonography in detecting appendicitis in a community hospitals. Am. J. Roentgenol., 184: 1809-1812.
PubMed - Friday, J.H., 2006. Update on appendicitis: Diagnosis and presurgical management. Curr. Opin. Pediatr., 18: 234-238.
PubMed - Fujii, Y., J. Hata, K. Futagami, T. Hamada and H. Mitsuoka et al., 2000. Ultrasonography improves diagnostic accuracy of acute appendicitis and provides cost saving to hospitals in Japan. J. Ultrasound Med., 19: 409-414.
PubMed - Himeno, S., S. Yasuda, Y. Oida, S. Mukoyama and T. Nishi et al., 2003. Ultrasonography for the diagnosis of acute appendicitis. Tokai J. Exp. Clin. Med., 28: 39-44.
PubMed - Khanal, B.R., M.A. Ansari and S. Pradhan, 2008. Accuracy of ultrasonography in the diagnosis of acute appendicitis. Kathmandu Univ. Med. J., 6: 70-74.
PubMed - Lee, J.H., Y.K. Jeong, K.B. Park, J.K. Park, A.K. Jeong and J.C. Hwang, 2005. Operator-dependent techniques for graded compression sonography to detect the appendix and diagnose acute appendicitis. Am. J. Roentgenol., 184: 91-97.
PubMed - Morin, M.J., 2008. Diagnosing acute appendicitis in adults. Am. J. Roentgenol., 191: W315-W315.
PubMed - Paulson, E.K., M.F. Kalady and T.N. Pappas, 2003. Clinical practice. Suspected appendicitis. New Engl. J. Med., 348: 236-242.
PubMed - Rompel, O., B. Huelsse, K. Bodenschatz, G. Reutter and K. Darge, 2006. Harmonic US imaging of appendicitis in children. Pediatr. Radiol., 36: 1257-1264.
PubMed - Styrated, J., T. Josephson and S. Eriksson, 2000. Reducing negative appendectomy: Evaluation of ultrasonography and computed tomography in acute appendicitis. Int. J. Qual. Health Care, 12: 65-68.
PubMed - Wiersma, F., B.R. Toorenvliet, J.L. Bloem, J.H. Allema and H.C. Holscher, 2009. US examination of the appendix in children with suspected appendicitis: The additional value of secondary signs. Eur. Radiol., 19: 455-461.
PubMed - Yamauchi, M., M. Miyamoto, K. Takeuchi and T. Fukuhara, 2008. Sonographic appearance of appendiceal diverticulitis. Intern. Med., 47: 1153-1154.
PubMed - Yu, S.H., C.B. Kim, J.W. Park, M.S. Kim and D.M. Radosevich, 2005. Ultrasonography in the diagnosis of appendicitis: Evaluation by meta-analysis. Korean J. Radiol., 6: 267-277.
PubMed - Zielke, A., H. Sitter, T. Rampp, T. Bohrer and M. Rothmund, 2001. Clinical decision-making, ultrasonography and scores for evaluation of suspected acute appendicitis. World J. Surg., 25: 578-584.
PubMed