
M.A. I. Chowdhury
M. T. Uddin
M. F. Ahmed
M. A. Ali
S.M. A. Rasul
M. A. Hoque
R. Alam
R. Sharmin
S. M. Uddin
M. S. Islam
Pakistan Journal of Biological Sciences
Year: 2006 | Volume: 9 | Issue: 9 | Page No.: 1617-1627







ABSTRACT
Untreated groundwater, often enriched in arsenic-one of the most important pollutants and trace elements of the aquatic system recently regarded as the major threat to drinking water-was and is being extensively used as a source of drinking for the decades in rural and semi-urban areas of the developing countries which results in a high incidence of arsenic with deleterious effects on humans and food chain. In Bangladesh, India, Vietnam and other developed countries, arsenic contamination in groundwater is considered to be the key environmental health problem of the twenty first century. In Bangladesh arsenic was first detected in the district of Chapai Nawabgonj bordering the West-Bengal district of India in 1993; since then higher levels of arsenic (exceeding the WHO standard of 0.01 mg L-1 and Bangladesh standard of 0.05 mg L-1) have been detected in many regions of the country including 61 districts out of 64. It is estimated that of the 140 million inhabitants of Bangladesh more than 100 million are at the risk of arsenic hazard, such arsenic hazards collapses the societal structure and socio-economic backbone of poor people of rural Bangladesh. The study tries to discuss the chronological extent and severity of the biggest global arsenic calamity prevailed in Bangladesh, socio-economic impact of arsenic hazard on the poor people of rural society living more than seventy percent under poverty limit in Bangladesh. Specially due consideration was given on the socio-economic impact on arsenic victims particularly earning male family member, young male, married female and young female going to be married as well as arsenic affected family and their interaction with non-arsenic-victim of the society.
PDF Abstract XML References Citation
How to cite this article
M.A. I. Chowdhury, M. T. Uddin, M. F. Ahmed, M. A. Ali, S.M. A. Rasul, M. A. Hoque, R. Alam, R. Sharmin, S. M. Uddin and M. S. Islam, 2006. Collapse of Socio-economic Base of Bangladesh by Arsenic Contamination in Groundwater. Pakistan Journal of Biological Sciences, 9: 1617-1627.
DOI: 10.3923/pjbs.2006.1617.1627
URL: https://scialert.net/abstract/?doi=pjbs.2006.1617.1627
DOI: 10.3923/pjbs.2006.1617.1627
URL: https://scialert.net/abstract/?doi=pjbs.2006.1617.1627
INTRODUCTION
Extensive arsenic contamination of groundwater has become a major disquiet where the water supply, predominantly rural water supply, is profoundly reliant on groundwater extracted from shallow aquifers and common trace of arsenic in drinking-water identified as a significant health risk (McNeill and Edwards, 1997; Pontius et al., 1994; Abernathy and Ohanian, 1993; Wu et al., 1989; Chen et al., 1988) and public health is severely endanger for its high toxicity and its ability to induce skin cancer after long term ingestion (Driehaus et al., 1998) leading to an inebitable socio-economic collapse of the poor rural society living more than seventy percent people under poverty limit. Recent studies indicate that arsenic in drinking water is a matter of great concern and is considered more dangerous than it was in the past because of the collapse of socio-economic backbone of the poor society specially in the developing countries. The current assessment, which is subjected to considerable debate, ranks arsenic in drinking water as a risk comparable to second-hand tobacco smoke and indoor radon gas causing sever social calamity to some extent although arsenic in drinking water was not detected as hazard even up to 1960. The occurrences of arsenic in groundwater environment has been reported in many places around the world particularly in Argentina (Nicolli et al., 1989; Smedley et al., 1998, 2001), Australia (Smith et al., 2003), Bangladesh (Karim, 2000; Nickson et al., 2000; Kinniburg and Smedley, 2001; McArther et al., 2001; Ravenscroft et al., 2001), Cambodia (Ahmed, 2003), Chile (Ahmed, 2003; Romero et al., 2003; Caceres et al., 1992), China (Inner Mongolia and Guizhou province) (Ahmed, 2003; Smedley et al., 2001), Hungary (Ahmed, 2003), India(West Bengal) (Battacharaya et al., 1997; Acharyya, 1999; Acharyya et al., 2000), Lao PDR (Ahmed, 2003), Mexico (Del Razo et al., 1990; Arminta et al., 1997), Mongolia (Ahmed, 2003), Nepal (Ahmed, 2003), Pakistan (Ahmed, 2003), Switzerland (Fabian et al., 2003), Taiwan (Kuo, 1968; Tsang et al., 1968; Chen et al., 1994; Guo et al., 1997), Thailand (Ahmed, 2003), the USA (Matisoff et al., 1982; Welch et al., 1988, 2000; Robertson, 1989; Peters et al., 1999; Schreiber et al., 2000) and Vietnam (Berg et al., 2001). Among them, arsenic contamination in groundwater of Bengal Delta including Bangladesh has been regarded not only as the severest natural catastrophe of the world but also collapses the social base of public society as a new social tragedy where more than 100 million people in 61 districts out of 64 are at the risk of severe arsenic hazard.
MATERIALS AND METHODS
Groundwater samples were collected from pre-selected tube-wells of the selected study areas and subsequently tested to determine the arsenic concentration in groundwater using fields kits, standard methods, Spectrophotometer, UV Spectrophotometer, AAS etc. Field kits were and are being used to determine arsenic content in groundwater of tube-wells in conducting rigorous water analysis in the field. Based on the concentration of arsenic, study were divided into mostly uncontaminated, uncontaminated, less-contaminated, sparsely contaminated, highly contaminated, severely contaminated and most severely contaminated area. Different types of questionnaire survey were conducted to evaluate the socio-economic impact of arsenic contamination on the poor rural society living more than seventy percent people under poverty limit in the study area. Socio-economic impact on arsenic victim specially earning male family member, young male, married female and young female going to be married as well as arsenic affected family and their interactions with non-arsenic victim of the society was investigated. Also relevant information and pertinent data were collected from other sources and analyzed subsequently to assess the severity of arsenic contamination. Socio-economic studies of arsenicosis were targetted to the poor people of three severely arsenic affected ares Samta of Jessore, Courtpara of Kushtia and Rajarampur of Nawabgang during 2002-2004.
RESULTS AND DISCUSSION
How does arsenic hazard extend in groundwater of Bangladesh?: In Bangladesh groundwater arsenic was first detected in the district of Chapai Nawabgang in 1993. Since then elevated levels of arsenic (exceeding the WHO standard of 0.01 mg L-1 and Bangladesh standard of 0.05 mg L-1) have been identified in many regions of the country (Ahmed et al. 1997; Khan et al., 1998; Talukder et al., 1998; Safiullah et al., 1998; Ahmed et al., 1998; Tanabe et al., 1998). Estimates of affected population are being updated, as more data are becoming available. According to Dave (1997), about 23 million people are at high risk endangered by arsenic in Bangladesh. Data on arsenic contamination in tube-well water gathered so far suggest that the presence of arsenic in groundwater is highly scattered in nature. At many places, tube-wells at relatively close proximity showed very different levels of arsenic concentrations. This makes it difficult to delineate the affected areas and to estimate the population at risk. So far arsenic contamination of groundwater has been detected in 41 out of 61 administrative districts and an estimated 35 million people in Bangladesh are at risk of arsenic toxicity (Khan et al., 1998). In accordance with survey findings of Dhaka Community Hospital (DCH) published in October 1997, 60 million people of 41 districts are at risk of arsenic contamination as water of tube-wells of 41 districts showed arsenic concentration above 0.05 mg L-1 (permissible limit of arsenic in drinking water for Bangladesh). According to a study report published jointly by the School of Environmental Sciences (SOES)of Jadabpur University of India and DCH, 50 million people of 29 districts of Bangladesh is at the risk of arsenic poisoning. Field survey conducted from August 95 to February 2000 by SOES and DCH shows that 100 million people of 54 districts of area 125,133 sq. km. Is at risk of arsenic hazard where groundwater of 73.39% of tubewells contain arsenic above 0.01 mg L-1 and 9.3 million people of 47 districts of area 112,407 sq. km. is at risk of arsenic poisoning where groundwater of 53.47% of tubewells contain above 0.05 mg L-1. (SOES and DCH, 2000). According to a recent estimate, 27% of shallow hand-tubewells have arsenic concentration exceeding 0.05 mg L-1; in acute arsenic problem areas more than 75% of shallow tubewells are contaminated with arsenic. Out of 64 administrative districts of Bangladesh, arsenic contamination has so far been reported in 61 districts. Arsenic problem alone has reduced the national safe water supply coverage by about 15 to 25%.
The extent of the arsenic problem can be described based on available field and laboratory analysis data. Although a very small number of wells have so far been tested compared to the total number of 7 to 8 million wells, it is possible to make an estimation about the probable arsenic contaminated wells based on the results of the large national surveys. Results from the DPHE/UNICEF field kit analysis, NRECA/ICDDRB Rural Electrification Board survey, DCH/SOES patient based surveys, BGS/DPHE national hydrochemical survey, UNICEF/INFS arsenicosis prevalence survey may be utilized to describe the extent.
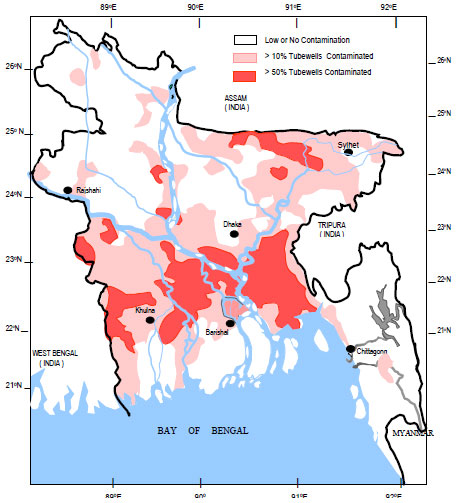 | |
| Fig. 1: | Arsenic contaminated areas in Bangladesh |
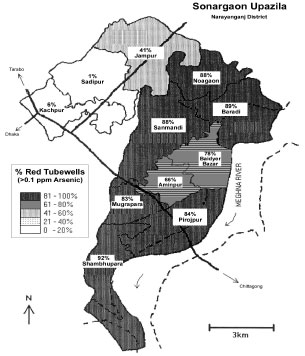 | |
| Fig. 2: | Union-wise arsenic distribution in Sonargaon upazila of Naryanganj district (Redrawn after BRAC, 2000) |
| Table 1: | National Arsenic Survey data based on Laboratory analyses (Ahmed, 2003) |
 | |
| Table 2: | Administrative areas with at least one tubewell exceeding drinking water standards |
 | |
Laboratory analyses by the NRECA, BGS/DPHE, DCH/SOES and UNICEF/INFS surveys (Table 1) shows that out of about 44,000 tested wells, 34% have arsenic concentrations of more than 0.05 mg L-1. Laboratory analyses conducted by different organizations such as BUET, BCSIR, BAEC etc., compiled in the BGS/MML (1999) report, show that about 35% of the wells have arsenic above 0.05 mg L-1.
Chandpur, Comilla, Laksmipur and Noakhali of chittagong division, Faridpur, Gopalganj, Munshiganj, Madaripur, narayangang, Shariatpur and Sherpur of Dhaka division, Jessore, Kushtia, Meherpur and Satkhira of Khulna division are the most arsenic contaminated areas of Bangladesh (Fig. 1). There is variability in the pattern of occurrences. In the North-west and South-west regions, contaminated and uncontaminated wells are located close to each other whereas in the South-east, particularly in Chandpur, almost all the shallow wells are contaminated. Testing of all wells using field kits conducted by BRAC, UNICEF and BAMWSP show large variations in the percentage of contaminated wells in different upazilas, e.g., almost 100% contamination in Hajiganj in Chandpur district compared to almost none contaminated in Porsha in Naogaon district (Ahmed, 2003).
There is large variability in the concentration ranges of arsenic within an area. In certain areas the concentration ranges show normal distribution pattern, whereas in other areas bimodal or polymodal distribution patterns are shown. There are variations in concentration ranges even in village scales where areas of low and high arsenic regions can occur as reported from Samta village of Sarsha thana of Jessore district (AAN, 1999). Very high concentrations can occur in a restricted area as found in Nawabgang Sadar of Chapai Nawabganj district, Charruppur of Iswardi of Pabna district, Gopalgng Sadar of Gopalgang district, Kachua, Hajigang and Faridgang of Chandpur district, Ramgang of Lakshmipur district, Begamgang of Noakhali district, Kushtia Sadar of Kushtia district, Sonargaon of Narayangang district, Sreenagar of Munshigang and Samta of Sharsha of Jessore district etc. (DPHE and BGS, 2000). These types of occurrences can be termed as hot spots.
Sonargaon is a severely contaminated upazilla under Narayangang district where all the wells have been tested by BRAC under a UNICEF/DPHE programme. The unionwise distribution of arsenic contaminated wells show that in eight unions most of the wells are contaminated (up to 89%) whereas in two unions only a small number of wells (>10%) are contaminated as shown in Fig. 2 (BRAC, 2000). The Dupi Tila sediments underlie these unions and most of the wells are developed there.
The study conducted by British Geological Survey (BGS), Department of Public Health Engineering (DPHE) and Mott MacDonald Limited (MML) in two phases examined 3534 distributed water samples from 61 districts except 3 hilly districts (DPHE, BGS and MML, 1999; BGS and DPHE, 2001) with an average of 58 samples per district and 8 samples per upazila. The study showed that arsenic concentration of 42% of all tubewell samples exceeded 10 μg L-1 and 25% exceeded 50 μg L-1. When only shallow tubewells are considered, 46 and 27% exceeded 10 and 50 μg L-1, respectively. In case of deep tubewell (> 150 m ) samples, arsenic content of only 5% exceeded 10 μg L-1 and 1% exceeded 50 μg L-1. The number of administrative areas with at least one sample exceeding Bangladesh Drinking Water Standard and WHO guideline value (BGS and DPHE, 2001) are shown in Table 2.
The percentages of shallow tubewells yielding water of various concentrations of arsenic prepared on the basis of BGS/DPHE test results are shown in Fig. 3 that provides information about the percentage of shallow tubewells producing water in excess of corresponding concentration.
 | |
| Fig. 3: | Levels of arsenic content in STW water |
Public health effected by arsenic contamination in Bangladeshi society: Health affects of arsenic termed as arsenicosis may be categorized to cancer effects and noncancer effects. The carcinogenic role of arsenic compounds was first noted over one hundred years ago in the Hutchinson (1887) observation that an unusual number of skin tumors developed in patients treated with arsenicals. In a 1980 review of arsenic, the International Agency for Research on Cancer (IARC, 1980) determined that inorganic compounds are skin and lung are carcinogens in humans via inhalation. Arsenic exposure also interferes with the action of enzymes, essential cations and transcriptional events in cells throughout the body and a multitude of multisystemic noncancer effects might ensue. Thounsands of poor rural people of Bangladesh living under proverty limit are severely attacked by both type of arsenicosis due to the long term exposure of arsenic contaminated water. As a result, the social scenario takes an ugly phase as the majority of arsenic patients in Bangladesh are unable to take proper treatment suffered by severe financial crisis and leads to the death day by day. A few clinical, large population based case-control epidermiological studies conducted by Tondel et al. (1999) identified a number of common arsenical manifestation and arsenic lesions such as different type of melanosis e.g., diffused melanosis, spotted melanosis, lucomelanosis, mucus membrane melanosis, different type of keratosis e.g., diffused keratosis, spotted keratosis, shyper keratosis, gangrene, squamoous cell carcinoma and hyperpigmentation in palms and soles and non-cirrhotic portal fibrosis among the population affected by arsenic in Bangladesh. In a later stage the patches might develop into cancer and foot will probably have to be amputated (Battacharaya et al., 1997; Quadiruzzaman, 1996; Pontius et al., 1994). Skin cancer, internal cancers of bladder, kidney, liver and lunges, neurological effects, hypertension, cardiovascular disease and diabetes mellitus, pulmonary disease and peripheral vascular disease are included to long-term health effects of exposure to arsenic (WHO, 2000). Characteristics skin lesions of arsenic toxicity indicates high exposure of arsenic which are distinctive in contrast to other clinical manifestations of arsenic intoxication including weakness, conjunctival congestion, edema, portal hypertension, bronchitis and hepatomegaly (Tondel et al., 1999; Mazumdar et al., 1992). Chowdhury et al., (2000) examined 11,180 people (including children) at random; they registered 2,736 (24.47%) people with arsenical skin lesions in 27 districts of Bangladesh, who usually drink water containing above 0.30 mg L-1 of arsenic. According to Tondel et al. (1999), in four villages of Faridpur, Narayangang, Nawabgang and Jessore district, arsenic concentration in groundwater ranged from 0.01 to 2.04 mg L-1 and the prevalence rate of arsenic lesions was 30.1 and 26.5% for males and female, respectively. An estimated 20 million people are exposed to the risk of arsenic related ailment through drinking of arsenic contaminated water in Bangladesh (BGS and MML, 1999). About 7,600 arsenic affected patients have so far been identified in arsenic affected areas. The arsenic problem has emerged as a big environmental disaster and more than 50 million people are exposed to arsenic above the Bangladesh drinking water standard (DPHE and BGS, 2000; DCH and SOES, 2000). DPHE, BGS and MML studies estimated that the population exposed to arsenic contamination would lie in the range 18.5-22.7 million ( DPHE, BGS and MML, 1999). Total populations exposed to above 0.01 mg L-1 and 0.05 mg L-1 in 43 districts in Bangladesh were 51 and 25 million, respectively (SOES and DCH, 2000). Based on upazila statistics the exposure levels to As exceeding 50 and 10 μg L-1 were 28.1 and 46.4 million, respectively (BGS and DPHE, 2001). Comparative scenario of total population exposed to arsenic risk in Bangladesh according to different sources is presented in Table 3.
Arsenic hazard causes social problems and breaks up societal ties: According to the reports of the national newspapers and other relevant sources, a significant number of people are attacked by arsenic lesions of which a few dies but the majority becomes the burden to the family and the society; obviously severe social hazard emerges in the arsenic affected areas; a large amounts of financial loss are being incurred by the individual publics and families as well as by the government for arsenic health hazard and setback of social structure.
| Table 3: | Total population exposed to arsenic contamination |
 | |
| Table 4: | Identification and treatment of arsenicosis |
 | |
| Table 5: | Nature of the treatment of arsenic patients in the study areas |
 | |
The arsenic contamination problem has triggered a number of social and societal problems that were unanticipated and are still not fully recognized. Recent studies confirm the fact that worst arsenic problems are encountered by the poorest fraction of the society (WHO, 2000)-particularly those who are already undernourished. Social fallout of arsenicosis is enormous. Some of the already identified social consequences of arsenicosis based on the socio-economic study are discussed.
Social instability: Arsenicosic causes extreme instability in social life of Bangladesh where people are confused and not able to get arsenic free drinking water. People are becoming dispirited without having proper treatment for arsenicosis. Case study shows that arsenicosis are not or seldom identified timely and even identified patient are not treated properly and timely due to only financial inability but also ignorance as shown in Table 4. Out of 75 identified arsenicosis patient, only 42 patients are treated of which 20 patients from Samta are treated where treatment rate is about 92%. Due to ignorance and proper knowledge of arsenicosis can not be identified within one year of exposure of the disease.
Socio-economic study evidents that public awareness play a vital role against arsenicosis. In Samta of Jessore, identification of arsenicosis and treatment of arsenicosis is much higher than other two districts due to the much motivation, involvement and activities of NGOs and donors; in Samta about 86% arsenicosis patients are treated by NGOs and donors but only 14% are by government treatment with no self treatment as shown in Table 5. In Rajarampur of Chapainawabgang and Courtpara of Kushtia arsenicosis treatment by NGOs and donor is very poor varying from 16.67 to 20% only where public motivation, involvement and activities of NGOs and donors are found very seldom; also self treatment of arsenicosis in Chapainawabgang is more than 3 times than Kushtia due to the better economic condition and financial status while self treatment in Samta of Jessore is almost nil due to very poor economic and financial condition.
Chaotic environment prevails due to people’s ignorance of arsenic in water, arsenicosis or why they are getting sick out of drinking water from tube well. Problem of arsenicosis is hampering the socialization of a child due to the fear of becoming a victim of arsenicosos is working as a barrier towards the proper psychological and physical development of a child. Arsenic is producing social stigmatization and discrimination. Social conflict over contaminated water is towards destroying social harmony and network relationships.
Superstition: Due to the ignorance of arsenic contamination and arsenicosis among the people in the remote villages, superstitions, prejudices and fairy tales are constructed surrounding arsenic patients. People stay away from arsenic victims, neglect or become scared of them due to such superstition. Some think of it as act of devil or evil spirits or impure air and keep themselves and their family members away from arsenic patients. Out of such prejudices many arsenic patients in the remote villages are passing miserable lives. Due to such superstition and prejudices 30 to 80% patients does not take any treatment as shown Table 6. In Samta of Jessore where more than 70% people are illiterate, tendency of superstition is the highest in the level of 80% while in Courtpara of Kushtia where about 65% public are literate, only 30% arsenic patient remain untreated due to superstition and 70% due to financial crisis.
| Table 6: | Reasons behind arsenic patients untreated in study areas |
 | |
Ostracism: Arsenic patients are often identified as patient of leprosy and remain ostracized (Mandal et al., 1998). Children of arsenicosis patients are not allowed to attend social and religious functions as well as are denied to take water from neighbor’s tube well. Arsenic victims are abandoned not only by society but also by their family members; in many cases husbands left wives or re-married and wives left their husbands temporarily for fear of being attacked by arsenicosis. None of the villagers keep contact with the patients or any member of their families or with their children; these families are not allowed to take bath in any of the village ponds, even people refrain from making new relationship with arsenic victim’s families. Such situation was found to be severe in North Rajarampur of Chapainawabgang where low-cast communities live in.
Diminish working ability: Arsenic gradually kills people. Dark spot on the skin, early symptom of arsenicosis, gradually turns to the nodules and become more pronounced depending on person’s exposure to water containing arsenic. Limbs can be affected by gangrene, internal organs including the liver, kidneys and lungs can be affected and in extreme cases cancer can occur in skin and internal organs. The victims become crippled and incapable of doing hard labor, gradually lose strength to move.
Marriage related problems: People become reluctant to establish marital relationship with those families suffering from arsenicosis giving birth to unlimited anxiety for parents of unmarried adult children. Arsenic victims are not able to find spouse; young woman and men are advised to remain unmarried. Like other problems divorce is also prevalent among arsenic victims; many couples live separately from their spouses, even many women are either getting divorce or becoming abandoned by their husbands. According to Socio-economic survey 3 couple of Rajarampur of Chapainawabgang district have been living separately from their spouses for more than one year, It is reported that 12 couple of 5 than as at Chapainawabgang district is living separately from their spouses (Bearak, 1998).
Impact on women: Like cooking, cleaning, feeding children and animals, woman play key role in water carrying. Women have no options, when supplies are limited, of contaminated water except for searching pure water from any source. Arsenic in tube wells often force woman to talk up to few Kilometers to get arsenic free water. They become burdened with additional responsibilities, which often force them to compromise with cultural ideology of parda. To cope with the crises of aresenicosis woman often play the key role not only through carrying arsenic free drinking water but also through providing nutritious food to the victims, drawing upon their savings, selling their very own assets and drawing upon network relationship (Sarkar, 1999).
Women are the worst victims of ostracism. They are doubly vulnerable: by the disease itself and by becoming excommunicated or outcast. Because arsenicosis like melanosis, spotted melalanosis, keratosis, ulcer Keratosis etc. change the complexions of victims and make them physically weak, these women’s marital tie becomes weaker (Sarker, 2001). Due to the socio-cultural position of women in society, unmarried women, women abandoned by husband and families live inhumanly. Woman suffering from arsenicosis are the most negligible among all victims of the disease. Due to the patriarchal nature of society women are abandoned, separated or divorced by their husbands. Concerned study conducted in Samta of Jessore, Rajarampur of Chapainawabgang and Courtpara of Kushtia involving 55 female victims at the verge of social violence reveals that women with arsenicosis are subject to domestic violence such as dowry ranging from 38.88% in Chapainawabgang to 42.85% in Kushtia, divorce ranging from 14.29% in Kushtia to 17.385% in Jessore, separation ranging from 14.29% in Kushtia to 17.385% in Jessore, desertion ranging from 8.7% in Jessore to 14.29% in Kushtia, physical torture ranging from 7.14% in Kushtia to 11.11% in Chapainwabgang and ploygomy ranging from 5.56% in Chapainwabgang to 7.14% in Kushtia as shown in Table 7.
On average women with arsenicosis are subject to social violence such as dowry 40%, divorce 16.36%, separation 16.36%, desertion 10.91%, physical torture 9.1% and ploygomy 7.27% as shown in percentile diagram of Fig. 4.
Relevant study conducted by Sarker (2001) showed that women with arsenicosis were subject to domestic violence such as dowry (41.7%), divorce (16.7%), separation (16.7%), desertion (8.3%), physical torture (8.3%) and ploygomy (8.3%).
| Table 7: | Effect of arsenicosis on women in terms of domestic violence |
 | |
| Table 8: | Domestic/Social violence compared with Sarker (2001) |
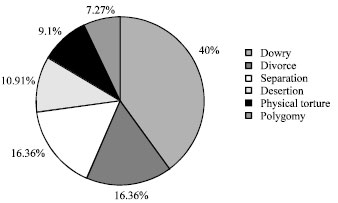 | |
| Fig. 4: | Pie-chart of arsenicosis on women in terms of domestic violence |
Findings of the concerned study can be well compared with Sarker (2001) as tabulated in Table 8.
Arsenicosis increases the economic burden of poor: Arsenicosis is more prevalent among the poor, who are forced to take contaminated tube well water and suffered with dietary deficiency affecting the toxicity of arsenic in human body due to the financial inability to buy arsenic free bottled water and nutritious food against arsenic toxicity. It is evident from the study that most of the people affected by arsenicosis are extremely poor. Lack of financial ability to get treatment for arsenicosos further deteriorate the condition of arsenic victims. Due to financial crisis, 20, 50 and 70% identified patients can not treated timely in Samta of Jessore, Rajarampur of Chapainawabgang and Courtpara of Kushtia as shown in Table 7. Spending huge money for treating arsenicosis increases the economic burden of poor. Moreover cost to obtain arsenic free drinking water also diminishes household income.
The poor victims become incapable of hard labor, which result into increasing poverty and continuous ill further compounded by social attitudes. Unfortunately arsenic victims are treated as untouchables and lose their jobs as arsenicosis acts as a barrier to have access to job for unemployed. As a result arsenic victims fail to contribute towards economic development of the country because they are refused work.
Yet another societal impact is that on livelihoods of families that lose head of household or “bread-earners” to the disease. There is a need for serious consideration of alternative livelihoods for people who may be affected by arsenicosis as well as for orphans and widows of those who pass away.
CONCLUSIONS
Arsenicosis due to taking of arsenic contaminated water collapses societal structure leading to enormous social fallout such as social instability, superstition, ostracism, diminishing working ability, marriage related problems, domestic violence to the women. Due to ignorance and proper knowledge of arsenicosis can not be identified within one year of exposure of the disease. Socio-economic study evidents that public awareness play a vital role against arsenicosis. Due to the ignorance of arsenic contamination and arsenicosis among the illiterate people in the remote villages, superstitions, prejudices and fairy tales are constructed surrounding arsenic patients and do not take treatment against arsenicosis. Arsenic patients are often identified as patient of leprosy and remain ostracized keeping them inactive in social activities. The arsenic victims become crippled and incapable of doing hard labor, gradually lose strength to move and ultimately leads to death. People become reluctant to establish marital relationship with arsenicosis patients and their families giving birth to unlimited anxiety for parents of unmarried adult children suffered by arsenicosis. On average women with arsenicosis are subject to social violence such as dowry around 40%, divorce 16%, separation 16%, desertion 9%, physical torture 8.5% and ploygomy 8%. Spending huge money for treating arsenicosis increases the economic burden of poor. Sometimes arsenic victim family lose head of the household or “bread-earners” due to the arsenicosis. Such kind of unavoidable social hazards signal arsenic contamination in groundwater as a looming disaster.
To tackle the social instability hailed from arsenicosis and to protect the collapse of socio-economic base of Bangladesh the following mesusre should be taken of.
| • | Identifying the causes of arsenic contamination; in this regard detection of source of arsenic in ground aquifer and release mechanism of arsenic from solid medium to liquid phase should get the priority to plan and design the proper remedial action against arsenic contamination. |
| • | Exploring for alternative safe water sources such as surface water sources like river, lake and ponds as well as rainwater harvesting. |
| • | Modification of drinking water standard, scientific research on arsenic contaminated water treatment technologies. |
| • | Identification of arsenic patients in the preliminary stage before long term exposure of arsenic. |
| • | Proper treatment of identified arsenic patients in time. |
| • | Improving nutrition facilities to arsenic patients and fighting against undernourishment. |
| • | Raising public awareness against arsenicosis, superstitions, prejudices and fairy tales etc. |
| • | Effective participation of the civil society in remedial measures against arsenic contamination and arsenicosis treatment. |
| • | Create suitable employment scope for the arsenic victim heads of the household or bread-earners. |
| • | Provide financial assistance and relief to the arsenic victim families specially arsenic victim females. |
REFERENCES
- Talukder, S.A., A. Chatterjee, J. Zheng and W. Kosmus, 1998. Studies of drinking water quality and arsenic calamity in groundwater of Bangladesh. Proceedings of the International Conference on Arsenic Pollution of Groundwater in Bangladesh: Causes, Effects and Remedies, February 8-12, 1998, Dhaka, Bangladesh.
- Tanabe, K., Y. Akiyoshi H. Yokota, H. Hironaka and S. Tsushima et al., 1998. Arsenic concentration of groundwater in Samta village and theapplicability of a field kit by Hironaka to quantify arsenic. Proceedings of the International Conference of Arsenic Pollution of Groundwater in Bangladesh: Causes, Effects and Remedies, February 8-12, 1998, Dhaka, Bangladesh.
- Tondel, M., M. Rahman, A. Magnuson, I.A. Chowdhury, M.H. Faruquee and S.A. Ahmad, 1999. The relationship of arsenic levels in drinking water and the prevalence rate of skin lesions in Bangladesh. Environ. Health Perspect., 107: 727-729.
PubMedDirect Link - Acharyya, S.K., S. Lahiri, B.C. Raymahashay and A. Bhowmik, 2000. Arsenic toxicity of groundwater in parts of Bengal basin in India and Bangladesh: The role of quaternary stratigraphy and holocene sea-level fluctuation. Environ. Geol., 39: 1127-1134.
Direct Link - Tsang, W.P., H.M. Chu, S.W. How, J.M. Fong, C.S. Lin and S. Yeh, 1968. Prevalance of skin cancer in an endemic area of chronic arsenicism in Tiwan. J. Natl. Cancer Inst., 40: 453-463.
PubMedDirect Link - Welch, A.H., M.S. Lico and J.L. Hughes, 1988. Arsenic in ground water of the Western United States. Ground Water, 26: 333-347.
Direct Link - Ahmed, K.M., R. Nickson, W.G. Burgess, J.M. Macarthur and M.B. Imam et al., 1998. On the release mechanism of Arsenic in groundwater of Bangladesh. Proceedings of the International Conference on Arsenic Pollution of Groundwater in Bangladesh: Causes, Effects and Remedies, Feb. 8-12, Dhaka, Bangladesh. pp: 120-129.
- Welch, A.H., D.B. Westjohn, D.R. Helsel and R.B. Wanty, 2000. Arsenic in the groundwater of the United States: Occurrence and geochemistry. Ground Water, 38: 589-604.
Direct Link - Arminta, M.A., R. Rodriguez and O. Cruz, 1997. Arsenic content in hair of people exposed to natural Arsenic polluted groundwater at Zimapan, Mexico. Bull. Environ. Contam. Toxicol., 9: 583-589.
CrossRefDirect Link - Wu, M.M., T.L. Kuo, Y.H. Hwang and C.J. Chen, 1989. Dose response relation between arsenic and well water and mortality from cancer. Am. J. Epidermol., 130: 1123-1132.
Direct Link - Battacharaya, P., D. Chatterjee and G. Jacks, 1997. Occurrence of Arsenic-contaminated groundwater in alluvial aquifers from delta plains, Eastern India: Options for safe drinking water supply. Water Resour. Dev., 13: 79-92.
Direct Link - Caceres, L., V.E. Gruttner and R. Conteras, 1992. Water recycking in arid region. Chilean case. Ambio, 21: 138-144.
Direct Link - Chen, C.J., T.L. Kuo, Y.H. Hwang and C.J. Chen, 1988. Arsenic and cancers. Lancet, 1: 414-415.
PubMedDirect Link - Chen, S.L., S.R. Dzeng, M.H. Yang, K.H. Chiau, G.M. Shieh and C.M. Wai, 1994. Arsenic species in groundwater of the Blackfoot disease areas, Taiwan. Environ. Sci. Technol., 28: 877-881.
CrossRefDirect Link - Chowdhury, T.R., B.K. Manal, G. Samanta, G.K. Basu and P.P. Chowdhury et al., 2000. Arsenic in Groundwater in Six Districts of West Bengal, India, the Biggest Arsenic Calamity in World, the Status Report up to August 1995. In: Arsenic Exposure and Health Effects, Chappell, W.R., C.O. Abernathy and R.L. Calderon (Eds.). Elsevier Science Ltd., UK., pp: 93-111.
- Del Razo, L.M., M.A. Arellano and M.E. Cebrian, 1990. The oxidation state of arsenic in well water from a chronic arsenicism area of Northern Mexico. Environ. Pollut., 64: 143-153.
PubMedDirect Link - Driehaus, W., M. Jekel and U. Hildebrandt, 1998. Granular ferric hydroxide. A new adsorbent for the removal of arsenic from natural water. Aqua, 47: 30-35.
Direct Link - Fabian, D., Z. Zhou, B. Wehrli and G. Friedl, 2003. Diagenetic cycling of arsenic in the sediments of eutrophic Bladeggersee, Switzerland. Applied Geochem., 18: 1497-1506.
CrossRefDirect Link - Guo, H.R., H.S. Chiang, H. Hu, S.R. Lipsitz and R.R. Monson, 1997. Arsenic in drinking water and incidence of urinary cancers. Epidemio, 8: 545-550.
Direct Link - Karim, M., 2000. Arsenic in groundwater and health problems in Bangladesh. Water Res., 34: 304-310.
Direct Link - Mandal, B.K., T.R. Chowdhury, G. Samanta, D.P. Mukherjee, C.R. Chanda, K.C. Saha and D. Chakraborti, 1996. Impact of safe water for drinking and cooking on five arsenic affected families for 2 years in West Bengal, India. Sci. Total Environ., 218: 185-201.
Direct Link - Matisoff, G., C.J. Khourey, J.F. Hall, A.W. Varnes and W.H. Strain, 1982. The nature and source of arsenic in North-eastern Ohio groundwater. Ground Water, 20: 446-456.
CrossRefDirect Link - Mazumdar, D.N.G., J. Dasgupta, A.K. Chakraborty, A. Chatterjee, D. Das and D. Chakraborty, 1992. Environmental Pollution and chronic arsenicosis in South Calcutta. Bull. WHO, 70: 481-485.
Direct Link - McArther, J.M., P. Ravenscroft, S. Safiullah and M. Thirlwall, 2001. Arsenic in groundwater: Testing pollution mechanism for sedimentary aquifers in Bangladesh. Water Resour. Res., 37: 109-117.
Direct Link - McNeill, S.L. and M. Edwards, 1997. Arsenic removal during precipitative softening. J. Environ. Eng. ASCE, 123: 453-460.
CrossRefDirect Link - Nickson, R.T., J.M. Mcarthur, P. Ravenscroft, W.G. Burgess and K.M. Ahamed, 2000. Mechanism of arsenic release to groundwater, Bangladesh and West Bengal. Applied Geochem., 15: 403-413.
CrossRefDirect Link - Nicolli, H.B., J.M. Suriano, G.M.A. Pearl, L.H. Ferpozzi and O.A. Baleani, 1989. Groundwater contamination with arsenic and other trace elements in an area of the Pampa, Province of Cordova, Argentina. Environ. Geol. Water Sci., 14: 3-16.
CrossRefDirect Link - Peters, S.C., J.D. Blum, B. Klaue and M.R. Karagus, 1999. Arsenic occurrence in new hamasphire drinking water. Environ. Sci. Technol., 33: 1328-1333.
CrossRefDirect Link - Pontius, F.W., K.G. Brown and C.J. Chen, 1994. Health implications of arsenic in drinking water. J. Am. Water Works Assoc., 86: 52-63.
Direct Link - Robertson, F.N., 1989. Arsenic in groundwater in oxidizing conditions South-west United States. Environ. Geochem. Health, 11: 171-185.
CrossRefDirect Link - Romero, L., H. Alonso, P. Campano, L. Fanfani and R. Cidu et al., 2003. Arsenic enrichment in waters and sediments of the Rio Loa (Second Region, Chile). Applied Geochem., 18: 1399-1416.
CrossRefDirect Link - Safiullah, S., A.K. Sarker, A. Zahid, M.Z. Islam and S.Z. Haider, 1998. Geochemical mapping and speciation of arsenic in the groundwater of faridpur municipality. Proceeding of the International Conference on Arsenic Pollution of Groundwater in Bangladesh: Causes, Effects and Remedies, Feb. 8-12, Dhaka, Bangladesh, pp: 94-96.
- Smith, J.V.S., J. Jankowski and J. Sammut, 2003. Vertical distribution of As (III) and As (V) in a coastal sandy aquifer: Factors controlling the concentration and speciation of arsenic in the stuarts point groundwater system, Northern New South Wales, Australian. Applied Geochem., 18: 1479-1496.
Direct Link - Berg, M., H.C. Tran, T.C. Nguyen, H.V. Pham, R. Schertenleib and W. Giger, 2001. Arsenic contamination of groundwater in Vietnam: A human health threat. Environ. Sci. Technol., 35: 2621-2626.
CrossRefDirect Link