
Vid Velikic
Medical University of Wien, 1090 Wien, Vienna, Austria
Mosad Zineldin
Department of Medicine and Optometry, Linnaeus University, 352 52 V�xj�, Sm�land, Sweden
LiveDNA: 46.33170
ORCID: 0000-0002-3055-1108
Ivana Dabovic
Medical University of Wien, 1090 Wien, Vienna, Austria
Fatma Mokhtar
Faculty of Medicine, Ain Shams University, Cairo Governorate, Egypt
Journal of Medical Sciences
Year: 2023 | Volume: 23 | Issue: 2 | Page No.: 38-44







ABSTRACT
Background and Objective: Depression and anxiety disorders (DAD) are the most prevalent mental disorders. Cognitive Behavioral Therapy (CBT) is an effective tool for treating different mental health conditions such as DAD. Patients’ involvement level in clinical decision-making (CDM) can affect and be affected by the different CBT modalities. The aim of this study was to investigate the effects of cognitive behavioral therapy on clinical decision-making. Materials and Methods: This study was conducted at the psychotherapeutic ward at the Clinical Division of Social-Psychiatry, Clinical Department of Psychiatry and Psychotherapy, Medical University of Vienna. As 100 patient diagnosed with anxiety and/or depressive disorders was included in the study. Multiple regression analysis was used for collecting predictors too. Results: Participation in integrated cognitive behavioral therapy (ICBT) had a positive effect of “empowerment”, in such a manner that allows patients to the feeling of influence in their life. An active and common style of participation was significantly more frequent at discharge than at admission. Female patients are more active in participating in shared clinical decision-making, compared to male patients. Conclusion: Providing DADs patients with patient self-efficacy training (PST), patient self-management (PSM) and knowledge increases their ability to be active participants in the clinical decision-making (CDM) process at admission when possible and at discharge.
PDF Abstract XML References Citation
Copyright: © 2023. This is an open access article distributed under the terms of the creative commons attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
How to cite this article
Vid Velikic, Mosad Zineldin, Ivana Dabovic and Fatma Mokhtar, 2023. The Effect of Integrated Cognitive Behavioral Therapy on Clinical Decision Making for Patients with Depression and Anxiety. Journal of Medical Sciences, 23: 38-44.
DOI: 10.3923/jms.2023.38.44
URL: https://scialert.net/abstract/?doi=jms.2023.38.44
DOI: 10.3923/jms.2023.38.44
URL: https://scialert.net/abstract/?doi=jms.2023.38.44
INTRODUCTION
Depression and anxiety disorders (DAD) are the most prevalent mental disorders1. Cognitive Behavioral Therapy (CBT) is an effective tool for treating different mental health conditions such as DAD. Although, Cognitive-Behavioral Therapy (CBT) and decision-making science are two vastly areas of study, they have integrated and emerged within the field of psychiatry and psychological sciences. Both address human knowledge, experience, information processing, cognition, behavior and the link between them2. The CBT is usually thought of as a temporary, problem-focused treatment focused on changing maladaptive emotional responses by altering patient’s ideas, actions, or both. The origin of CBT dates back partially to the hypotheses of early researchers such as B.F. Skinner and Joseph Wolpe, who excelled the behavioral therapy movement in the 19503.
Cognitive restructuring is a strategy in which clinicians facilitate patients to identify, evaluate and modify inaccurate or unhelpful thinking related to emotional distress. Both patients’ involvement level in clinical decision-making (CDM) and different CBT modalities alter each other.
Integrated cognitive behavioral therapy (ICBT) is the integration of patient self-efficacy (PSE) and patient self-management (PSM) with clinical Cognitive Behavioral Therapy (CBT), which is recommended to improve long-term treatment and prevention methods. An ICBT goal is enabling individuals to control their actions, attitudes, feelings and emotional intelligence by activating or deactivating their behavior to enhance their activities with positive reinforcement compared to decreasing their activities with negative reinforcement4. Note that patients who have difficulty in activation are unable to increase their activities. Thus, supporting them in a softer manner is recommended by, for example, encouraging them to try to improve their self-efficacy and self-management skills while coaching them to manipulate small tasks and then gradually increase their actions to assure their behavioral regulation and activation abilities. Problem-solving allows patients to systematically approach and address their life problems via cognitive and behavioral techniques5.
According to a large population-based survey, up to 33.7% of people are suffering from an anxiety disorder6, with the median age of onset being eleven to fourteen years7. Anxiety disorders and depression frequently coexist, which may contribute to the severity of the clinical picture. Depression, a mental disorder, affects peoples’ deas, behavior, motivation, emotions and sense of well-being8. Several hypotheses about pathophysiology of depression exists, including monoamine hypothesis, genetic, environmental, endocrine factors and neurogenesis9. According to DSM-IV, the average lifetime prevalence of depression is 12.8%, while the 12-month prevalence is 5.7% with the female: Male ratio 2:110. Some severe cases of depression can include suicidal thoughts11. A study, published almost 30 years ago, predicted that depression will represent the main cause of impairment in everyday life by the year 202012.
The DADs are highly comorbid and correlate with each other13. Zineldin14 found that the correlation between anxiety and depression is unquestionable as their symptoms are among the most disabling, influencing the overall health and Quality of Life (QoL). Thus, called them both together as DEPXITY psychiatric illness. Both anxiety and depression (DEPXITY) reflect a similar emotional state and both are related to suicide risk. Thus, DEPXITY is considered as one disease with different symptoms because it affects the patients’ sense of wellbeing, hence QoL14,15.
Innovative, patient-centered care approaches have emerged to incorporate patient health priorities, goals, preferences and shared decision making, in particular, older adults with multiple conditions such as anxiety and depression16-18. Zineldin19 found that patient self-efficacy (PSE) training approach which is a construct grounded in social cognitive theory enhances patients’ self-confidence to believe that they are capable of being more active in clinical decision making related to the cognitive behavior therapy program at admission and discharge. Integrating patient self-management (PSM) should be a part of CBT because it enables patients to deal with their disease and to control one’s own life19 hence, regulating their behavior4. This also make patients believe that they are capable of being actively participating in making clinical decisions, even in adverse situations14. The core idea of this method of self-management therapy (SMT) is to allow participants to switch on and/or off their actions and behavior. A vital advantage of the SMT in behavioral activation is enabling and encouraging patients to continuously take actions and make decisions that will yield better results to them, hence improve their QoL.
Manuals-based self-help therapies may be utilized for treating DADs. These techniques commonly include training of relaxation, emotional awareness, acceptance and commitment as well as breathing. Moreover, they are also applicable for treating mild and transient episodes of depression, preferably incorporated with physical activity.
However, Cognitive Behavioral Therapy (CBT) is considered the gold standard treatment of anxiety disorders. This also applies to the treatment of the moderate depression, while more severe cases of anxiety and depression may also benefit from CBT, preferably in combination with antidepressants20.
Despite these efforts, many cognitive behavior clinicians still face challenges with incorporating patients in making clinical care planning decisions. Many patients prefer to be passive in joining the clinical decision making related to their conditions. Thus, the aim of this study was to investigate the effects of Cognitive Behavioral Therapy (CBT) on clinical decision-making (CDM).
MATERIALS AND METHODS
Study area: This study was performed at the University Clinic of Psychiatry and Psychotherapy/Department of Social Psychiatry, at Vienna General Hospital. The data was collected between October, 2016 and September, 2019.
Sample size: The study was performed on 100 patients (62.2% female, 35.1% male and 2.7% unspecified) and according to the ethical permit number 1809/2014 of the Medical University of Vienna.
Statistical analysis: A clinical assessment conducted at our clinic resulted in depression and anxiety disorder diagnosis according to the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10)21 On one hand, patients diagnosed with depression (57% of all patients) were suffering from light or moderate depression. On the other hand, the patients diagnosed with an anxiety disorder (66% of all patients) were mostly suffering from General Anxiety Disorder (GAD), social phobia, agoraphobia and Obsessive-Compulsive Disorder (OCD). Half of all participating patients were taking medications besides cognitive behavioral therapy. The most frequent drugs that have been used were sertraline (up to 100 mg/day) and escitalopram (up to 20 mg/day). The participants were recruited after receiving information about the study and giving their written consent. The participation included completion of the questionnaires prior to and after seven week-long treatments with CBT. The patients were interviewed using the following questionnaires (translated into German, of note, all participants were either native speakers or fluent in written and spoken German):
| • | CEDAR (Clinical decision making and outcome in routine Care for People with Severe Mental Illness)-CDIS (Clinical decision-making involvement and satisfaction) standardized questionnaire |
| • | Morisky medication adherence scale |
| • | Helping alliance questionnaire 1984 |
| • | Illness perception questionnaire |
CDIS (Clinical decision-making involvement and satisfaction): Questionnaire about patient’s satisfaction regarding made decisions22. Illness perception questionnaire: Measures patients’ beliefs and feelings about their illnesses23. It also measures patient personal control, self-efficacy (PSE) and self-management (PSM) (e.g. It is important for me to know all the side effects of my treatment, I should make my own decisions concerning I do everyday problems connected to my illness, I can determine whether my illness gets better or worse and I have the power to influence my illness, my actions will have no effect on the outcome of my illness. There is nothing which can help my condition, I have a clear picture or understanding of my condition my illness does (not) worry me.
Morisky medication adherence scale: Designed to estimate the risk of medication non-adherence24.
In the t-test dropouts and completers were compared. Changes in quality of life-score, symptoms of depression, or symptoms of anxiety were collected and evaluated using regression analysis. Independent variables were social data, the severity of anxiety/depression at the beginning/admission, other psychiatric disorders and a few somatic symptoms.
Ethical approval
Institutional review board statements: This study was conducted in accordance with the Declaration of Helsinki. No experiments on human or animals were implemented. The work was authored according to Good Scientific Practice ethics in science and research guidelines of the Medical University of Vienna.
Statement of informed consent: Informed consent was obtained from the patient(s) for their anonymized information to be publish.
RESULTS
The study revealed that there was no significant association (p>0.05) between the way of clinical decision making, PSE, PSM and the characteristics age (rs = 0.01, p = 0.96), therapeutic relationship (rs = 0.21, p = 0.25) and the subjective cause of illness “y own behaviour” (rs = 0.01, p = 1.00).
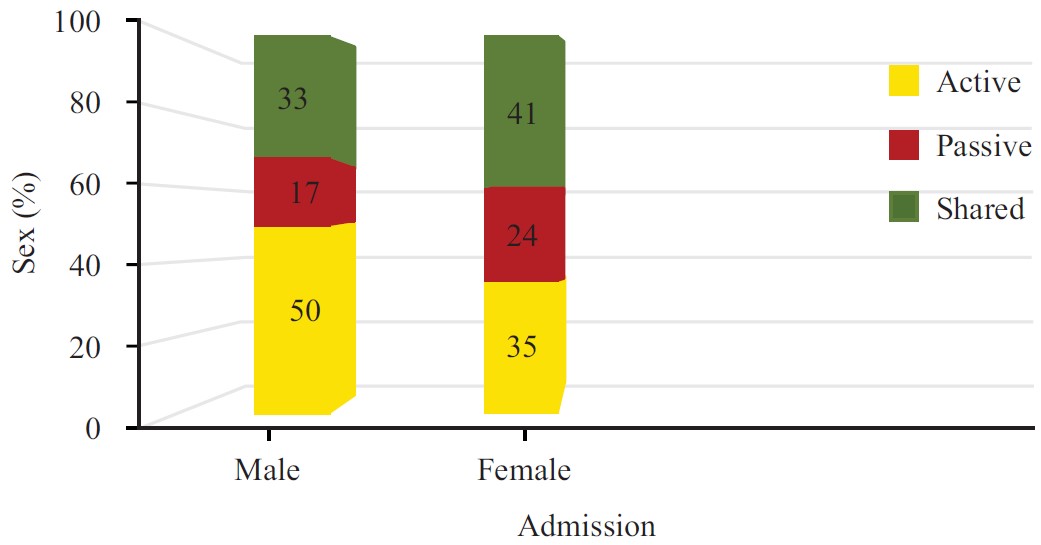 |
| Fig. 1: | Clinical decision making at the time of admission. Patients are divided based on their sex |
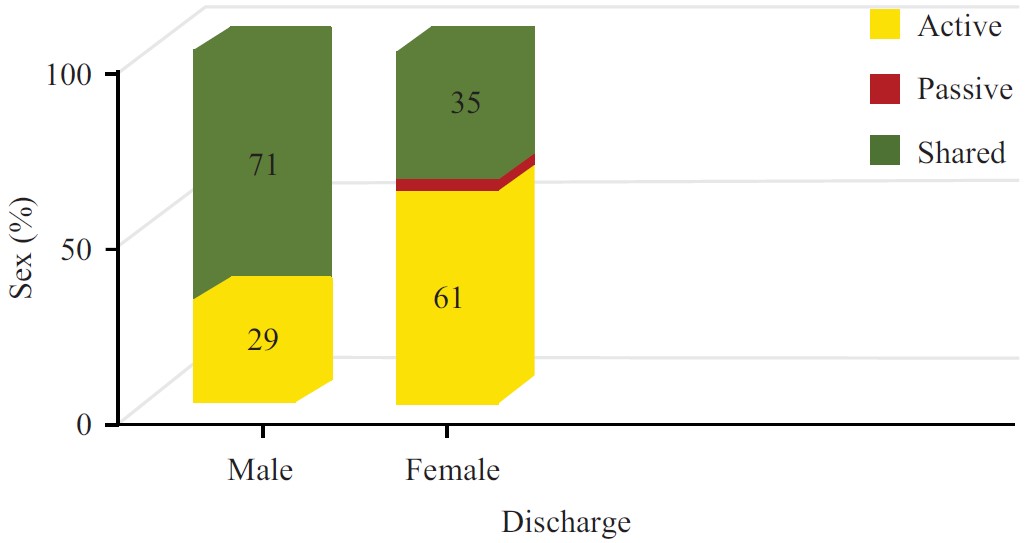 |
| Fig. 2: | Clinical decision making at the time of discharge |
Of the sample, 66% have anxiety disorders and 57% have depressive disorders. Women tended to have more self-efficacy and sharing in clinical decision making (41% compared to 33% of men) or passive (24% compared to 17% of men) style of participation when admitted compared to men who chose half an active style of relationship (50% compared to 35% of women Fig. 1).
Female patients with AD (anxiety disorder) showed less PSE and PSM because they were more passive (25%) and shared decision-making (42%) participation style in clinical decision-making at admission, whereas female patients without AD showed better PSE and PSM because they were a predominantly active (53%) participation in decision making style. As shown in Fig. 2, at discharge, women tended to be more active (61% compared to 29% of men) (4% compared to 0% of men), compared to men. Of note, at discharge, patients with an AD showed a predominantly active (54%) participation style and patients without an AD showed a mutual (57%) participation style. The passive participation style was hardly present in patients with or without AD at discharge. No differences were made between patients with single (either DD or AD) or dual diagnosis.
Most patients without a DD (depressive disorder) showed better PSE and PSM because they were active in decision participation style at discharge (61%) compared to patients with a DD who predominantly (54%) showed a common participation style, there was no significant change since admission. The search for predictors showed that there was a tendency towards a mutual or active participation style at the time of admission among patients with a rather positive attitude towards medications. Half of our patients have been taking medications (62% sertraline and 38% escitalopram). There was also a tendency towards a common or active participation style at the time of admission and discharge if patients regarded “their personality” less strongly as the cause of the disease but other factors (genetics, environment). The tendency towards a common or active participation style in the clinical decision was further reported by patients with “greater satisfaction with the therapeutic relationship”.
Taken together, results showed that participation in integrated clinical behavior therapy (ICBT) had an effect of “empowerment”, an active and mutual style of participation was significantly more frequent at discharge than at admission. Women were more likely to show a passive and mutual participation style at admission, but almost exclusively an active or mutual participation style at discharge.
The opposite was for male participants, who predominantly reported an active participation style at the time of admission, but a majority mutual participation style at discharge. Patients with anxiety disorders, regardless of gender, reported a more passive and mutual participation style at the time of admission but after completing the cognitive behavioral therapy program, most of these patients actively participated in the clinical decision. Patients with DD showed a rather passive style at the time of admission but exhibited a shared style at the time of discharge.
DISCUSSION
According to the results, at the time of the discharge active and shared decision-making styles occurred on significantly more occasions in comparison to the time of admission. The study assumed that such an outcome is a consequence of increased confidence between patients and staff during the treatment period. Additionally, female patients are even more prone to active and shared decision making, than male patients. Such discrepancy between genders could be explained with the fact that staff at the healthcare setting were predominantly female. This could impact the patients decision-making preferences. This result was constant with Schuttner et al.18 arguing that many physicians consider patient values, health priorities and preferences influential during clinical decision-making. Also, healthcare sittings staff values can affect patient health priorities, goals and decision making before, during and aftercare planning16.
Integrated cognitive behavioral therapy (ICBT) with patient’s self-efficacy (PSE) and patient self-management (PSM) can be as effective as medication in treating anxiety and depression disorder and might aid in cases where medication alone is ineffective. Skills that patients acquire in ICBT are useful, practical and helpful strategies that can be incorporated into everyday life to help them cope better with future stressors and difficulties, even after the treatment ends. This was consistent with what Zineldin19 found that too much control by others on one’s own life, such as solely making decision for the patients can be a significant factor correlating with depression. Internal control over own personal life and health such as PSE, PSM and sharing the clinical decision making was a significant factor to ameliorate or control some of the negative symptoms of anxiety. Self-efficacy is also vital factors in ICBT. Some previous studies argue that patient quality of life could be improved by effective self-efficacy training and management16,17,25,26. Thus, enhanced performance and patient self-management (PSM) and performance in personal life is a shared positive impact to adjust both depression (DEP) and anxiety (XITY)27. His study shows that DEPXITY is associated with negative life quality. In contrast to the previous studies describing the correlation between CDM and race, emotions, nursing, etc. Our study is innovative and describes the phenomenon that was previously overlooked by scholars.
Limitations and future recommendation: Discomfort and nervousness could be felt at the beginning of CBT/ICBT, because it consists of facing the root of problems.
Staff at the healthcare setting were predominantly female. This could impact the patients’ decision-making preferences.
One of the main recommendations of this study is to provide patients with DADs with a patient self-efficacy training (PST) and knowledge to increase their ability to be active participant in the clinical decision-making process at both of the admission when possible and at the discharge. Having trained psychiatrists and the patient’s will to collaborate will help overcome the limitation of discomfort and nervousness, thus this type of therapy can be very successful and useful for further life.
CONCLUSION
Participating in an integrated clinical behavior therapy (ICBT) lead to “empowerment”, an active and mutual style of participation was significantly more frequent at discharge than at admission. Active style in making decisions is very important for the patients, because they have the feeling of influence on their quality of life. Besides medications, cognitive behavioral therapy has shown positive influence in patients with anxiety and/or depression disorder and their willing to participate in clinical decision making. We always have to be aware that people with mental illness are indeed among the most stigmatized, marginalized and vulnerable members of the society. According to current observation this type of therapy is generally effective not only for the healing process but also in clinical decision making. To benefit from the CBT program and ICBT patients need to collaborate with doctors and other medical staff. It is very important to encourage more medical students to start a career in psychiatry, as previous studies have shown lack of interest in the past years worldwide. Well trained psychiatrists are crucial part for the further developing of this program. The psychiatrists and all other medical staff working with patients suffering from depression and/or anxiety disorder should be confident about this program.
SIGNIFICANCE STATEMENT
This study was done to investigate the effects of Integrated cognitive behavioral therapy (ICBT) on clinical decision-making (CDM). Taken together, results showed that participation in integrated clinical behavior therapy (ICBT) had an effect of “empowerment”, an active and mutual style of participation was significantly more frequent at discharge than at admission. Besides medications, ICBT has shown a more positive influence on patients with anxiety and/or depression disorder and their willing to participate in clinical decision making. According to our ICBT type of therapy is comprehensive effective then CBT, not only for the healing process, but also in the case of clinical decision making.
REFERENCES
- Chisholm, D., K. Sweeny, P. Sheehan, B. Rasmussen, F. Smit, P. Cuijpers and S. Saxena, 2016. Scaling-up treatment of depression and anxiety: A global return on investment analysis. Lancet Psychiatry, 3: 415-424.
CrossRefDirect Link - Leddy, M.A., B.L. Anderson and J. Schulkin, 2013. Cognitive-behavioral therapy and decision science. New Ideas Psychol., 31: 173-183.
CrossRefDirect Link - Kaczkurkin, A.N. and E.B. Foa, 2015. Cognitive-behavioral therapy for anxiety disorders: An update on the empirical evidence. Dialogues Clin. Neurosci., 17: 337-346.
CrossRefDirect Link - Hirano, M., K. Ogura, M. Kitahara, D. Sakamoto and H. Shimoyama, 2017. Designing behavioral self-regulation application for preventive personal mental healthcare. Health Psychol. Open, Vol. 4.
CrossRefDirect Link - Wenzel, A., 2017. Basic strategies of cognitive behavioral therapy. Psychiatric Clin. N. Am., 40: 597-609.
CrossRefDirect Link - Bandelow, B. and S. Michaelis, 2015. Epidemiology of anxiety disorders in the 21st century. Dialogues Clin. Neurosci., 17: 327-335.
CrossRefPubMedDirect Link - Auerbach, R.P., P. Mortier, R. Bruffaerts, J. Alonso and C. Benjet et al., 2018. WHO world mental health surveys international college student project: Prevalence and distribution of mental disorders. J. Abnormal Psychol., 127: 623-638.
CrossRefDirect Link - van der Feltz‐Cornelis, C., S.F. Allen, R.I.G. Holt, R. Roberts, A. Nouwen and N. Sartorius, 2021. Treatment for comorbid depressive disorder or subthreshold depression in diabetes mellitus: Systematic review and meta-analysis. Brain Behav., Vol. 11.
CrossRefDirect Link - Jesulola, E., P. Micalos and I.J. Baguley, 2018. Understanding the pathophysiology of depression: From monoamines to the neurogenesis hypothesis model - are we there yet? Behav. Brain Res., 341: 79-90.
CrossRefDirect Link - Bromet, E., L.H. Andrade, I. Hwang, N.A. Sampson and J. Alonso et al., 2011. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med., Vol. 9.
CrossRefDirect Link - Friedman, E.S. and I.M. Anderson, 2014. Handbook of Depression. 2nd Edn., Springer Healthcare Tarporley, Cham, ISBN: 978-1-907673-78-8, Pages: 105.
CrossRefDirect Link - Murray, C.J.L. and A.D. Lopez, 1996. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020. Harvard School of Public Health, Boston, USA, ISBN: 9780965546607, Pages: 43.
Direct Link - Kalin, N.H., 2020. The critical relationship between anxiety and depression. Am. J. Psychiatry, 177: 365-367.
CrossRefDirect Link - Zineldin, M., 2021. Neurological and psychological determinants of depression, anxiety, and life quality. Int. J. Preventive Med., Vol. 12.
CrossRefDirect Link - Beiske, A.G., E. Svensson, I. Sandanger, B. Czujko, E.D. Pedersen, J.H. Aarseth and K.M. Myhr, 2008. Depression and anxiety amongst multiple sclerosis patients. Eur. J. Neurol., 15: 239-245.
CrossRefDirect Link - Tinetti, M.E., A.D. Naik, L. Dindo, D.M. Costello and J. Esterson et al., 2019. Association of patient priorities-aligned decision-making with patient outcomes and ambulatory health care burden among older adults with multiple chronic conditions: A nonrandomized clinical trial. JAMA Intern. Med., 179: 1688-1697.
CrossRefDirect Link - Freytag, J., L. Dindo, A. Catic, A.L. Johnson and A.B. Amspoker et al., 2020. Feasibility of clinicians aligning health care with patient priorities in geriatrics ambulatory care. J. Am. Geriatrics Soc., 68: 2112-2116.
CrossRefDirect Link - Schuttner, L., J.R. Lee, S.H. Sherlock, J.D. Ralston and A.M. Rosland et al., 2022. Primary care physician perspectives on the influence of patient values, health priorities, and preferences on clinical decision-making for complex patients with multimorbidity: A qualitative study. Risk Manage. Healthcare Policy, 15: 2135-2146.
CrossRefDirect Link - Zineldin, M., 2021. Stress, anxiety and patient self-efficacy. J. Res. Med. Sci., 26: 540-541.
Direct Link - Seeliger, J., T. Lenz and M. Nickel, 2008. Patient with double depression in inpatient psychosomatic treatment. Psychiatr. Psychotherapie, Vol. 4.
CrossRefDirect Link - WHO., 2004. International Statistical Classification of Diseases and Related Health Problems. 2nd Edn., World Health Organization, Rome, ISBN: 9241546530, Pages: 125.
Direct Link - Puschner, B., T. Becker, B. Mayer, H. Jordan and M. Maj et al., 2016. Clinical decision making and outcome in the routine care of people with severe mental illness across Europe (CEDAR). Epidemiol. Psychiatric Sci., 25: 69-79.
CrossRefDirect Link - Weinman, J., K.J. Petrie, R. Moss-Morris and R. Horne, 1996. The illness perception questionnaire: A new method for assessing the cognitive representation of illness. Psychol. Health, 11: 431-445.
CrossRefDirect Link - Morisky, D.E., L.W. Green and D.M. Levine, 1986. Concurrent and predictive validity of a self-reported measure of medication adherence. Med. Care, 24: 67-74.
PubMedDirect Link - Peters, M., C.M. Potter, L. Kelly and R. Fitzpatrick, 2019. Self-efficacy and health-related quality of life: A cross-sectional study of primary care patients with multi-morbidity. Health Qual. Life Outcomes, Vol. 17.
CrossRefDirect Link - Wallace, E., C. Salisbury, B. Guthrie, C. Lewis, T. Fahey and S.M. Smith, 2015. Managing patients with multimorbidity in primary care. BMJ, Vol. 350.
CrossRefDirect Link - Carman, K.L., P. Dardess, M. Maurer, S. Sofaer, K. Adams, C. Bechtel and J. Sweeney, 2013. Patient and family engagement: A framework for understanding the elements and developing interventions and policies. Health Aff., 32: 223-231.
CrossRefDirect Link