
Mohammed Mahmoud
Department of Internal Medicine, Medical Research Division, National Research Centre, Cairo, Egypt
Safinaz El-Tokhy
Department of Medical Biochemistry, Medical Research Division, National Research Centre, Cairo, Egypt
Dalia El-Lebedy
Department of Clinical and Chemical Pathology, Medical Research Division, National Research Centre, Cairo, Egypt
Mohammed Abu Elfotouh
El-Tawfik Military Clinics, Cairo, Egypt
Ghada H. El-Arabi
Ministry of Health, Egypt
Journal of Medical Sciences
Year: 2013 | Volume: 13 | Issue: 5 | Page No.: 353-359







ABSTRACT
DNA fragmentation in peripheral blood lymphocytes is a reliable marker for oxidative stress occurring in the liver of chronic hepatitis C (CHC) patients which reflects a direct genotoxic effect of the virus and suggests a same genotoxic effect that might operate in the liver. Previous studies have investigated DNA damage in peripheral leukocytes of CHC patients, but none focused on genotype 4. This work aimed at examining DNA damage in different treatment outcomes of genotype 4 infection. The study included 80 viral hepatitis C genotype 4 patients and 80 healthy volunteers. HCV-RNA was detected by real-time PCR, genotype was defined by INNO-LiPA and DNA damage was assayed using alkaline Comet assay. The mean percentage of DNA damage was significantly higher in patients' group than in control group (p<0.01) and in null response (48.75±11.12) and breakthrough response (49.33±1.03) patients than in SVR patients (22.78±13.95) (p<0.05/3). Comet results revealed that all breakthrough and null response patients have DNA damage. Interestingly, 78.5% of SVR patients had DNA damage (64.3% showed mild damage and 14.2% showed marked damage). In conclusion, in genotype 4; despite clearance of serum HCV-RNA and apparent clinical resolution; SVR patients might not experience infection clearance and should be followed up being at suspected risk for virus reactivation.
PDF Abstract XML References Citation
Received: March 30, 2013;
Accepted: April 15, 2013;
Published: June 13, 2013
How to cite this article
Mohammed Mahmoud, Safinaz El-Tokhy, Dalia El-Lebedy, Mohammed Abu Elfotouh and Ghada H. El-Arabi, 2013. Peripheral Blood Lymphocytes' DNA Damage in Different Treatment Outcomes of Chronic Viral C Hepatitis Genotype 4 Infection. Journal of Medical Sciences, 13: 353-359.
DOI: 10.3923/jms.2013.353.359
URL: https://scialert.net/abstract/?doi=jms.2013.353.359
DOI: 10.3923/jms.2013.353.359
URL: https://scialert.net/abstract/?doi=jms.2013.353.359
INTRODUCTION
Hepatitis C virus (HCV) infection is prevalent in approximately 2% of the world's population (Dustin and Rice, 2007). Egypt has the highest epidemic of HCV in the world, with a recent estimated prevalence of 14.7% (DeWolfe Millera and Abu-Raddad, 2010) and genotype 4 is the predominant genotype affecting up to 91% of the patients (El-Ray et al., 2010).
Recently, HCV infection has been characterized by an increased oxidative stress in the peripheral blood mononuclear cells and liver (La Vignera et al., 2012). DNA fragmentation in peripheral blood lymphocytes is a reliable marker for oxidative stress occurring in the liver of chronic hepatitis C patients (Bolukbas et al., 2006), it reflects a direct genotoxic effect of the virus and suggests that the same genotoxic effect may operate in the liver and contribute to hepatocarcinogenesis (Grossi et al., 2008).
DNA damage assay in the peripheral blood lymphocytes is the least invasive and low number of cells is required to measure DNA lesions (Loft and Poulsen, 1999). The Comet assay is one of the useful methods to quantify DNA damage and has been exploited as a laboratory measure of genotoxicity in human bio-monitoring and clinical studies (Kassie et al., 2000; McKenna et al., 2008).
The current standard treatment of chronic HCV infection, a combination of pegylated interferon and ribavirin, has been reported to have the best overall sustained response rate in 55% of patients. However, clinical results obtained from several trials on genotype 4 have been inconsistent (Esmat and Abdel Fattah, 2009).
Previous clinical studies have investigated DNA damage in peripheral leukocytes associated with chronic viral C hepatitis with none focused on genotype 4, this work aimed at studying peripheral blood lymphocytes DNA damage in different treatment outcomes of chronic viral C hepatitis genotype 4 infection using alkaline Comet assay.
MATERIALS AND METHODS
Subjects: Eighty viral hepatitis C genotype 4 patients, who were enrolled for interferon therapy protocol, were included in the present study. They were recruited from hepatology clinics of the General Health Insurance Authority Polyclinics. Their combined therapy was a fixed weekly dose of 160 μg of 20 KD linear pegylated interferon α-2a and ribavirin in standard and adjusted doses for 48 weeks (El-Ray et al., 2010; Esmat and Abdel Fattah, 2009). Patients were fully informed in advance about the nature of our study and gave informed consents. The study protocol was approved by the ethical committee of the National Research Center.
According to their response to interferon therapy, they were divided into 3 groups. Sustained virologic response (SVR) group including 28 subjects, SVR was defined by undetectable HCV-RNA in serum 24 weeks after combined therapy withdrawal (Welker and Zeuzem, 2009). Null Response group including 26 patients, Null response was defined by <2 log (10) reduction in HCV-RNA after 12 weeks treatment (Chayama et al., 2012). The breakthrough group including 26 patients, breakthrough response is defined when HCV-RNA rebounds and becomes detectable before treatment is completed (Sherman et al., 2007), all patients in this group received only 24 weeks of interferon therapy. Eighty age, sex and culture matched healthy volunteers who were negative for HCV antibodies were enrolled as a control group. All subjects were evaluated clinically and exclusion criteria included: history of antioxidants administration for a month preceding the study, alcohol intake, smoking, chronic diseases and any other liver diseases or co-infections.
Laboratory methodology: Venous blood samples were withdrawn from all subjects included in the study. Serum was separated and assayed for liver function tests: AST (aspartate transaminase), ALT (alanine transaminase), ALP (alkaline phosphatase), total bilirubin and albumin using Olympus auto-analyzer AU-400 (Olympus Diagnostica, Japan). Prothrombin Time (PT) was assayed and International Normalized Ratio (INR) was calculated for each subject. Hemoglobin %, total leukocyte and platelet counts were measured using Hematology auto-analyzer (Abbott Cell Dyn CD-1700). HCV-RNA was detected by real time-PCR and the genotype was defined by the reverse line probe assay (INNO-LiPA). Peripheral blood lymphocytes DNA damage was assayed using alkaline Comet assay (single-cell microgel electrophoresis technique).
Detection of HCV-RNA by real time-PCR and HCV Genotyping: Viral RNA was extracted from patients' plasma using the QIAamp Viral RNA Kit (Qiagen Hilden, Germany, Cat No. 52904) according to the manufacturer's protocol. HCV- RNA was detected by COBAS Amplicor HCV Kit (Roche Diagnostic Systems, NJ, USA) with a lower limit of detection: 18 IU/mL. HCV genotype was defined by the reverse line probe assay (INNO-LiPA v.1.0, innogenetics, Ghent, Belgium) according to the manufacturer’s instructions.
Assessment of DNA damage by alkaline comet assay
Cell preparation: Peripheral blood lymphocytes were isolated from heparinized blood samples within a maximum 2 h period after collection by centrifugation over Ficoll hypaque density gradient (Pharmacia LKB Biotechnology, Piscataway, NJ, USA). After centrifugation, peripheral blood lymphocytes represented as a buffy coat were gently aspirated and washed twice by Phosphate Buffered Saline (PBS) at pH 7.4.
Preparation of cell microgels on slides: All the procedures of the alkaline Comet assay (Singh et al., 1988; Blasiak et al., 2003) were done at low temperature to minimize spontaneous DNA damage. Fully frosted slides were covered with 1% Normal Melting Point (NMP) agarose (Sigma). After solidification, the gel was scraped off the slide and cell microgels were prepared on the slides as layers. The first layer of gel was made by coating the slides with 0.7% NMP agarose (Sigma). When this layer had solidified at 4°C, a second layer containing the separated peripheral blood lymphocytes mixed with 0.6% Low Melting Point (LMP) agarose (Sigma) was placed on the slides. After 10 min solidification on ice, a final layer of 0.6% LMP agarose was added.
Cell Lysis, DNA unwinding, gel electrophoresis and DNA staining: Afterwards the slides were immersed for 1 h in ice-cold freshly prepared lysis solution (2.5M NaCl, 100 mM Na2EDTA, 10 mM Tris-HCl, 1% Na hydroxide (Sigma), pH 10) with 1% Triton X-100 (Sigma) and 10% dimethyl sulfoxide (DMSO), added fresh to lyse cells and allow DNA unfolding.
Then, the slides were placed in a horizontal gel electrophoresis chamber filled with fresh electrophoresis buffer (300 mM NaOH, 1 mM Na2EDTA, pH 13.0) for 20 min at 4°C to allow DNA unwinding and expression of alkali-labile sites.
Denaturation and electrophoresis were performed at 4°C under dim light. Electrophoresis was carried out for 30 min at 300 mA. After electrophoresis the slides were rinsed gently three times with a neutralization buffer (0.4 M Tris-HCl, pH 7.5) to remove excess alkali and detergents. Each slide was stained with ethidium bromide (10 μg mL-1) then cover slipped and stored at 4°C until analysis.
Visualization and analysis of comet: The slides were examined at 400x magnification using a fluorescence microscope (IX70; Olympus, Tokyo, Japan) equipped with an excitation filter of 549 nm and a barrier filter of 590 nm, attached to a digital camera (Olympus) with high resolution. A damaged cell is visualized as each cell had the appearance of a comet, with a brightly fluorescent head and a tail to one side formed by the DNA containing strand breaks that were drawn away during electrophoresis. Normal undamaged cell was visualized as an intact DNA without any protrusions. Samples were analyzed by counting the number of damaged cells out of 100 cells per slide to calculate the percentage (%) of DNA damage.
Interpretation: Genotoxicity is expressed as visual score in a range of 0-100 that can be classified into groups (Azqueta et al., 2009; Moller, 2006). In the present study, we categorized DNA damage into 3 groups (1) mild damage>0 and<25%, (2) moderate damage 25-50% and marked damage>50%. Comet tail formation was also documented, the extent of comet tail formation is proportional to DNA damage present and selected as the best parameter that reflects DNA damage (Collins, 2004; Trzeciak et al., 2008).
Statistical analysis: Data was analysed using the statistical package for social science (SPSS software version 16, Chicago, Illinois). Data was presented as Mean±standard deviation (SD). Non-parametric variables were compared by the Kruskal-wallis one-way analysis of variance with Post Hoc analysis using a Mann-Whitney U test. Parametric variables were compared using Student's t test and one-way analysis of variance with Post-Hoc analysis. Differences were considered significant at 0.05/3 for comparisons made by Kruskal-Wallis one-way analysis of variance, otherwise at p<0.05.
RESULTS
The demographic and laboratory data of all studied subjects are summarized in Table 1. There was no statistically significant difference between different groups with respect to age and sex (p>0.05). HCV-RNA was detected in all patients of null and breakthrough response, while all SVR subjects were negative for it.
Serum ALT and AST were significantly higher in patients' group than in control group (p = 0.03). The SVR patients had lower ALT and AST levels than the non-SVR patients (p<0.05/3). There was no significant difference regarding the same parameters on comparing the null response patients to breakthrough response patients. Serum ALP and total bilirubin levels were significantly higher in breakthrough response patients than in control group (p = 0.02).
As regards hematological findings, SVR patients had higher platelet count than the non-SVR patients (p<0.05/3). Breakthrough patients had significantly lower hemoglobin % and platelet count than control subjects (p = 0.03). No statistical significant differences were observed regarding the mean levels of albumin, PT, total leukocyte count among different studied groups.
| Table 1: | Demographic and laboratory data of different studied groups |
 | |
| Data presented as Mean±SD, *p<0.05 vs control, § p<0.05/3 vs. null and breakthrough groups, SVR: Sustained virologic response, AST: Aspartate transaminase, ALT: Alanine transaminase, ALP: Alkaline phosphatase, PT: Prothrombin time, INR: International normalized ratio, Hb: Hemoglobin, TLC: Total leukocyte count, PLT: Platelet count | |
| Table 2: | Descriptive analysis of DNA damage in different groups |
 | |
| †SVR: Sustained virologic response | |
 | |
| Fig. 1: | The mean percentage of peripheral blood lymphocytes DNA damage in different studied groups |
The mean percentage of DNA damage was significantly higher in patients' group than in control group (p<0.01) and in null response (48.75±11.12) and breakthrough response (49.33±1.03) patients than in SVR patients (22.78±13.95) (p<0.05/3) (Fig. 1). However, no statistically significant difference was found on comparing the null with the breakthrough groups. Descriptive analysis of DNA damage in different groups is shown in Table 2.
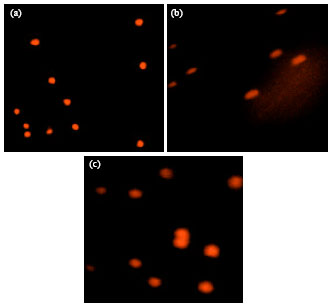 | |
| Fig. 2(a-c): | DNA damage by Comet assay, Images are visualized by the digital camera fitted fluorescent microscope, (a) An intact DNA in normal subjects, (b) High degree of DNA damage clarified by a slightly pointed end due to the migration of fragmented DNA through electrophoresis (tailed) and (c) Moderate DNA damage as revealed by less tightly intact DNA due to slight damage (non-tailed) |
Comet assay clarified an intact DNA in the control group (Fig. 2a). Meanwhile, all breakthrough and null response patients showed DNA damage; 100% of breakthrough patients had moderate DNA damage, 61.5% of null response patients had moderate damage while 38.5% had marked damage. Both breakthrough and null response groups clarified a well defined comet tail formation (Fig. 2b). Interestingly, only 21.5% of SVR patients showed intact DNA, while 78.5% showed DNA damage; of which in 64.3% it was mild and in 14.2% it was marked, with no comet tail formation (Fig. 2c).
DISCUSSION
HCV infection is implicated in the development of hepatocellular carcinoma (HCC). The virus induces double-strand DNA breaks and enhances the mutation frequency of proto-oncogenes and tumor suppressors (Machida et al., 2010) which may lead to inflammation-related carcinogenesis (Murata et al., 2012).
An increased oxidative stress in chronic hepatitis C patients due to the continuous generation of Reactive Oxygen Species (ROS) and reactive nitrogen species in Kupffer cells and polymorphonuclear cells in the liver as well as systemic oxidative stress secondary to hepatic oxidative stress has been reported (La Vignera et al., 2012). The use of antioxidant and antiviral therapies can reverse these deleterious effects of HCV in part by inhibiting ROS induction by HCV and restoring the function of the DNA repair enzymes, respectively (Pal et al., 2010).
Although hepatocytes are the primary sites of viral replication, HCV is potentially lymphotropic, invading and propagating in lymphocytes which are differentially implicated in the active forms of CHC (Bhargava et al., 2011). DNA fragmentation in peripheral blood lymphocytes of CHC patients is a reliable marker for oxidative stress occurring in the liver (Bolukbas et al., 2006).
In this study, we investigated the occurrence of peripheral blood lymphocytes DNA fragmentation in different clinical outcomes of interferon therapy in patients with chronic viral hepatitis genotype 4. In order to quantify the degree of DNA damage, we used the alkaline Comet assay which is very sensitive well-established genotoxicity test and a good biomarker of induced DNA damage (Kassie et al., 2000; McKenna et al., 2008).
Our results showed that SVR group had lower ALT levels, AST and higher platelet count than the non-SVR group. Similar findings were reported by Sanefuji et al. (2009). Comet analysis revealed that CHC patient groups had a significant higher DNA damage than the control group. Both the Null and the breakthrough response groups which represent the failure of the interferon therapy in our patients showed higher DNA damage than the SVR group which represents the clinical resolution of virus. Both breakthrough and Null response patients had high degrees of DNA damage with comet tail formation, coinciding with their studied liver function tests which denote activity of CHC.
Our SVR patients had a significant DNA damage compared to control subjects. In SVR group, 64.3% had mild DNA damage and 14.2% had marked damage. These findings point strongly that the interferon therapy in SVR patients did not provide complete pathophysiological cure.
In a previous study done by Radkowski et al. (2005), HCV- RNA has been detected in the livers of patients who have achieved a sustained virologic response to antiviral therapy. Also, Castillo et al. (2006) reported that HCV persists and replicates in the liver and peripheral blood mononuclear cells of most SVR responders for years after normalization of liver enzyme levels and clearance of serum HCV-RNA. A plausible explanation may be the newly reported issue of occult hepatitis C infection (Bhargava et al., 2011), in which both hepatocytes and lymphocytes are differentially implicated. Though it's an occult state, it induces DNA damage (Deng et al., 2008) and is associated with increased risk of developing HCC (Bhargava et al., 2011).
Radkowski et al. (2005) reported that HCV RNA may persist in liver or macrophages and lymphocytes in patients with SVR and this continuous viral presence could result in persistence of humoral and cellular immunity for many years after therapy and could present a potential risk for infection reactivation.
Furthermore, Sanefuji et al. (2009) declared that recurrent HCC still developed after the curative hepatectomy, even if viral elimination had been successful. In 12.5% of cases with SVR, HCV-RNA was detected in the non-cancerous tissue and immunohistochemistry revealed overexpression of p53 in 100% of HCCs from SVR patients. He suggested that molecular alterations in hepatocarcinogenesis of SVR patients might be different from those of CHC patients.
CONCLUSION
In conclusion, CHC genotype 4 patients who are non responders to combined pegylated interferon/ribavirin therapy, namely the null and the breakthrough responders, have a high degree of DNA damage. Also, SVR patients have DNA damage but to a lesser degree. Suggesting that despite clearance of serum HCV- RNA and apparent clinical disease resolution, SVR patients might not experience HCV infection clearance and should be followed up being at suspected risk for virus reactivation.
REFERENCES
- Azqueta, A., Y. Lorenzo and A.R. Collins, 2009. In vitro comet assay for DNA repair: A warning concerning application to cultured cells. Mutagenesis, 24: 379-381.
PubMed - Bhargava, A., G. Raghuram, N. Pathak, S. Varshney, S. Jatawa, D. Jain and P.K. Mishra, 2011. Occult hepatitis C virus elicits mitochondrial oxidative stress in lymphocytes and triggers PI3-kinase-mediated DNA damage response. Free Radic. Biol. Med., 51: 1806-1814.
PubMed - Blasiak, J., E. Gloc, K. Wozniak, J. Drzewoski, M. Zadrozny and T. Pertynski, 2003. Free radicals scavengers can differentially modulate the genotoxicity of amsacrine in normal and cancer cells. Mutat. Res., 535: 25-34.
PubMed - Bolukbas, C., F. Bolukbas, A. Kocyigit, M. Aslan, S. Selek, M. Bitiren and M. Ulukanligil, 2006. Relationship between levels of DNA damage in lymphocytes and histopathological severity of chronic hepatitis C and various clinical forms of hepatitis B. J. Gastroenterol. Hepatol., 21: 610-616.
PubMed - Castillo, I., E. Rodriguez-Inigo, J.M. Lopez-Alcorocho, M. Pardo, J. Bartolome and V. Carreno, 2006. Hepatitis C virus replicates in the liver of patients who have a sustained response to antiviral treatment. Clin. Infect. Dis., 15: 1277-1283.
PubMed - Chayama, K., S. Takahashi, J. Toyota, Y. Karino and K. Ikeda et al., 2012. Dual therapy with the nonstructural protein 5A inhibitor, daclatasvir, and the nonstructural protein 3 protease inhibitor, asunaprevir, in hepatitis C virus genotype 1b-infected null responders. Hepatology, 55: 742-748.
PubMed - Collins, A.R., 2004. The comet assay for DNA damage and repair: Principles, applications and limitations. Mol. Biotechnol., 26: 249-261.
CrossRefPubMedDirect Link - Deng, L., T. Adachi, K. Kitayama, Y. Bungyoku and S. Kitazawa et al., 2008. Hepatitis C virus infection induces apoptosis through a Bax-triggered, mitochondrion-mediated, caspase 3-dependent pathway. J. Virol., 82: 10375-10385.
PubMed - DeWolfe Millera, F. and L.J. Abu-Raddad, 2010. Evidence of intense ongoing endemic transmission of hepatitis C virus in Egypt. Proc. Natl. Acad. Sci. USA., 107: 14757-14762.
Direct Link - Dustin, L.B. and C.M. Rice, 2007. Flying under the radar: The immunobiology of hepatitis C. Annu. Rev. Immunol., 25: 71-99.
PubMed - Esmat, G. and S. Abdel Fattah, 2009. Evaluation of a novel pegylated interferon alpha-2a (Reiferon Retard ®) in Egyptian patients with chronic hepatitis C genotype 4. Digest. Liver Disease, 3: 17-19.
Direct Link - Grossi, S., A. Sumberaz, M. Gozma, F. Matiolli, G. Testino and A. Martelli, 2008. DNA damage in peripheral blood lymphocytes of patients with cirrhosis related to alcohol abuse or to hepatitis B and C viruses. Eur. J. Gastroenterol. Hepatol., 20: 22-25.
PubMed - Kassie, F., W. Parzefall and S. Knasmuller, 2000. Single cell gel electrophoresis assay: A new technique for human biomonitoring studies. Mutat. Res., 463: 13-31.
PubMed - La Vignera, S., R.A. Condorelli, E. Vicari, R. D'Agata, A.E. Calogero, 2012. Sperm DNA damage in patients with chronic viral C hepatitis. Eur. J. Intern. Med., 23: e19-E24.
PubMed - Loft, S. and H.E. Poulsen, 1999. Markers of oxidative damage to DNA: Antioxidants and molecular damage. Meth. Enzymol., 300: 166-184.
PubMed - Machida, K., H. Tsukamoto, J. Liu, Y. Han and S. Govindarajan et al., 2010. c-Jun mediates HCV hepatocarcinogenesis through STAT3 andnitric oxide-dependent impairment of oxidative DNA repair. Hepatology, 52: 480-492.
PubMed - Moller, P., 2006. The alkaline comet assay: Towards validation in biomonitory of DNA damaging exposures. Basic Clin. Pharmacol. Toxicol., 98: 336-345.
PubMed - Murata, M., R. Thanan, N. Ma and S. Kawanishi, 2012. Role of Nitrative and Oxidative DNA damage ininflammation-related carcinogenesis. J. Biomed. Biotechnol.
CrossRefDirect Link - Pal, S., S.J. Polyak, N. Bano, W.C. Qiu and R.L. Carithers et al., 2010. Hepatitis C virus induces oxidative stress, DNA damage and modulates the DNA repair enzyme NEIL1. J. Gastroenterol. Hepatol., 25: 627-634.
PubMed - Radkowski, M., J.F. Gallegos-Orozco, J. Jablonska, T.V. Colby and B Walewska-Zielecka et al. 2005. Persistence of hepatitis C virus in patients successfully treated for chronic hepatitis C. Hepatology, 41: 106-114.
PubMed - Sanefuji, K., H. Kayashima, T. Iguchi, K. Sugimachi and Y. Yamashita et al., 2009. Characterization of hepatocellular carcinoma developed after achieving sustained virological response to interferon therapy for hepatitis C. J. Surg. Oncol., 99: 32-37.
PubMed - Sherman, K.E., R. Fleischer, K. Laessig, J. Murray, W. Tauber and D. Birnkrant, 2007. Development of novel agents for the treatment of chronic hepatitis C infection: summary of the FDA Antiviral Products Advisory Committee recommendations. Hepatology, 46: 2014-2020.
PubMed - Singh, N.P., M.T. McCoy, R.R. Tice and E.L. Schneider, 1988. A simple technique for quantitation of low levels of DNA damage in individual cells. Exp. Cell Res., 175: 184-191.
CrossRefPubMedDirect Link - El-Ray, A., R. Moucari, M. El-Ghannam, A.A. Taha and M.A. Saber et al., 2010. Insulin resistance: A major predictor of significant liver fibrosis in egyptian patients with genotype 4 chronic hepatitis C. J. Hepatol., 52: S409-S409.
CrossRef - Trzeciak, A.R., J. Barnes and M.K. Evans, 2008. A modified alkaline comet assay for measuring DNA repair capacity in human populations. Radiat Res., 169: 110-121.
PubMed - Welker, M.W. and S. Zeuzem, 2009. Occult hepatitis C: how convincing are the current data? Hepatology, 49: 665-675.
PubMed