
Md. Hassan M. Ahmed
Department of Anesthesia and ENT Surgery, Faculty of Medicine,
Asian Network for Scientific Information Cairo University, Egypt
Md. Ehab H. Abu-Zaid
Department of Anesthesia and ENT Surgery, Faculty of Medicine,
Asian Network for Scientific Information Cairo University, Egypt
Journal of Medical Sciences
Year: 2007 | Volume: 7 | Issue: 8 | Page No.: 1297-1303







ABSTRACT
The present study evaluated the effect of bilateral endoscopic Sphenopalatine Ganglion Block (SPGB) combined with General Anesthesia (GA) for sinonasal surgery with respect to the blood loss, isoflurane consumption, hypotensive agent used, recovery time, postoperative pain and postoperative complications. Thirty patients were randomly allocated to receive GA alone (non-block group, n = 15) or combined GA and SPGB (block group, 15). The Mean Arterial Pressure (MAP) intraoperatively was maintained at 55-60 mm Hg. The consumption of isoflurane and the frequency of esmolol use were evaluated in both groups. The recovery time was recorded. A scoring system named Postoperative Respiratory System Evaluation Scoring (PRSES), was formed for evaluation of postoperative respiratory complications The pain intensity, postoperative tramadol consumption in both groups were also assessed. Intraoperatively, the isoflurane consumption was less in block group (p<0.001). The number of patients requiring esmolol was significantly higher in non-block group. Recovery time was longer in non-block group. PRSESs in all evaluation times were better in block group. In the PACU the total tramadol consumption was significantly reduced in block group (p≤0.005). Postoperative pain scores were lower in block group until 150 min. Other postoperative complications were more frequent in non-block group at all evaluation times. Bilateral SPGB combined with GA is effective in reducing blood loss, isoflurane consumption, hypotensive agent use, postoperative PRSESs 2-5, other complications, tramadol consumption and postoperative pain intensity in sinonasal surgery and associated with better recovery profiles and accepted surgeon and patient satisfaction.
PDF Abstract XML References Citation
How to cite this article
Md. Hassan M. Ahmed and Md. Ehab H. Abu-Zaid, 2007. Role of Intraoperative Endoscopic Sphenopalatine Ganglion Block in Sinonasal Surgery. Journal of Medical Sciences, 7: 1297-1303.
DOI: 10.3923/jms.2007.1297.1303
URL: https://scialert.net/abstract/?doi=jms.2007.1297.1303
DOI: 10.3923/jms.2007.1297.1303
URL: https://scialert.net/abstract/?doi=jms.2007.1297.1303
INTRODUCTION
Endoscopic sinus surgery became a popular method for treatment of many nasosinus problems. The endoscope has afforded direct visualization of critical landmarks and greater ease of instrumentation to remove disease from areas most commonly responsible for pathogenesis of sinusitis (McLaughlin, 2001). Although inhaled anesthesia alone is used for surgery, it is desirable to have an additional technique (including regional blocks) to maintain low blood pressure, reduce blood loss and reduce the anesthetic requirements and to attenuate the possible postoperative complications including pain. (Higashizawa and Koga, 2001).
Postoperative pain continues to be an important problem, despite the availability of potent and rapidly acting analgesic agents. Although sinonasal surgery is now among the most common head and neck surgical procedures, pain after sinonasal surgery have not been fully controlled. However, information on the severity and duration of the pain that a patient can expect to experience after sinonasal surgery is of tremendous importance. It can enable better patient counseling, allowing patients to be more prepared for the postoperative experience and possibly improving outcome (Friedman et al., 1996).
Regional block is supposed to be effective adjuvant to general anesthesia during sinonasal surgery. There are many regional techniques including topical or infiltration of local anesthetics, infraorbital nerve block and nasociliary block (Higashizawa and Koga, 2001; Molliex et al., 1996; Danielsen, 1992; Rice, 1989; Lee et al., 1997).
The Sphenopalatine Ganglion (SPG) has somatosensory effects through the trigeminal and facial nerves, visceral motor functions through its parasympathetic activity via the superficial petrosal nerve and sympathetic functions through its connection to the cervical sympathetic chain via deep petrosal nerve. The principal sensory distribution is to the orbit, nose, palate and buccal mucosa (Cambareri, 1997). The blockade of this ganglion has been used to treat headache and facial pain. There are many approaches to block this ganglion, the most recent one being the transnasal Endoscopic injection approach (Prasanna and Murthy, 1993a, b; Koshy and Varghese, 1999).
The analgesic efficacy of the ganglion block although well documented (Varghese and Koshy, 2001; Janzen and Scudds, 1997) is yet to receive few studies (Friedman et al., 1996; Hwang et al., 2003) about its usefulness intraoperatively or postoperatively during or after sinonasal surgery. A literature search reveals only two studies, one studied the effect of bupivacaine when applied topically to block SPG on postoperative pain following endoscopic sinus surgery (Friedman et al., 1996) and the other studied the effect of SPGB before removal of nasal packing (Hwang et al., 2003).
The present study was designed to evaluate the efficacy of SPGB combined with general anesthesia in patients undergoing FESS with or without septoplasty (sinonasal surgery) as regard the blood loss, isoflurane consumption, postoperative pain and analgesic need.
MATERIALS AND METHODS
Following Local Ethical Committee Approval, 30 ASA physical status I and II patients undergoing functional endoscopic sinus surgery with or without septoplasty (sinonasal surgery) were studied at Cairo university hospital (Kasr EL-Aini) from December 2004 to December 2006. All patients gave informed consent before participating in the study. Patients receiving cardiovascularly active drugs or drugs influencing blood coagulation were excluded from the study. Patients entering the study were randomly assigned to receive either General Anesthesia (GA) alone (Non-block group) or GA combined with Sphenopalatine ganglion block (SPGB) (Block group).
Preoperatively, patients were instructed in the use of Visual Analog Scale (VAS) for pain (O = No pain, 10 = most severe pain). All patients received a standard premedication of midazolam 2 mg IV 30 min prior to surgery. Anesthesia was induced with propofol 2 mg kg-1, fentanyl 2 μg kg-1. Atracurium 0.5 mg kg-1 to facilitate tracheal intubation with a cuffed endotracheal tube. Oropharyngeal pack inserted. Lungs were ventilated to maintain the PaCO2 within 35 mm Hg. Anesthesia was maintained with 100% O2 and isoflurane 1% end-tidal. All patients received lactated ringers at 3 mL kg-1 and were placed in a 15° reverse trendlenburg position to improve venous drainage. After achieving satisfactory level of anesthesia, patients were subjected to SPGB. In patients of the GA alone, normal saline was injected in the same way as combined group. Neither the anesthetists nor the surgeons were informed either local anesthetic or normal saline was given. In both groups, 0.5% lidocaine containing a 200,000 fold dilution of epinephrine was injected into the nasal mucosa to induce vasoconstriction and local anesthesia around the incisional area.
Bilateral sphenopalatine ganglion block: The technique includes topical anesthesia to the nasal mucosa between the middle and inferior turbinates from nares to the nasopharynx, followed by a needle insertion in the same tract guided by rigid nasal endoscope for blocking agent injection to the ganglion.
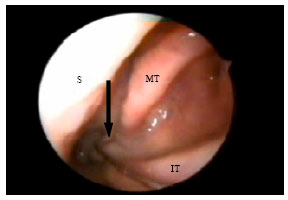 | |
| Fig. 1: | Under endoscopic control (4 mm, 30°), long, 20-gauge needle is inserted in mucosa just behind and over middle turbinate tail, seeking sphenopalatine foramen; MT = Middle Turbinate; IT = Inferior Turbinate; S = Septum |
 | |
| Fig. 2: | Surgical anatomy of region. (A) Location of sphenopalatine foramen. with detailed magnification of window indicated in A (bone of palatine processes has been removed) and some simplified details of anatomy of sphenopalatine fossa. Sphenopalatine artery is anterior and superior to sphenopalatine ganglion, so needle (arrowed) should be inserted anteroposteriorly into inferior portion of sphenopalatine foramen, pointing upward |
The nasal cavity, between the middle and inferior turbinates, from nares to posterolateral wall of the nasopharynx was anesthetized topically with 5% lidocaine + 1:200,000 epinephrine using cotton-tipped applicators. This passage was sterilized by an additional cotton-tipped applicator soaked with iodine solution. A 20-gauge/5-inch spinal needle was used for the transnasal injection. The exposed needle tip was bent along the port side with a sterile needle-holder to form a 45° angle, so that the side port indicator on the hub became a tip pointer. The needle was lubricated with 5% lidocaine jelly, inserted into the anesthetized nasal meatus and advanced with the bevel mark facing laterally. When the tip of the needle came in contact with the posterolateral wall of the nasopharynx just posterior to the posteroinferior end of middle turbinate, the needle was pushed into the posterolateral nasopharyngeal mucosa with the tip pointer facing laterally. After negative aspiration, 1.5 mL of 0.5% bupivacaine was injected. The needle was flushed and removed. A dry cotton-tipped applicator was inserted down to assure no bleeding after needle removal. The precise localization of the SPG area was achieved using 30° nasal endoscopes (Fig. 1) (Felisati et al., 2006).
Anatomical localization of the ganglion: An important landmark is the constant convergence of some of the vessels of lateral nasal wall towards the SP foramen due to the disappearance of the vessels into the foramen. This point is called vanishing point. SPG is the largest group of neurons in the head and neck. SP foramen, which leads to the SPG, lies immediately behind the ethmoidal crest situated at the posterior end of the attachment of the middle turbinate, oriented at an angle 15-20° with the sagittal plane. The superior turbinate acts as a pointer to the SPG and it is 12 mm above and lateral to the superior border of the Choana. (Fig. 2) SPG is situated in the pterygopalatine fossa. Medial to it, is the SP foremen, which transmits the SP vessels and nerves from pterygopalatine fossa to the nose. The ganglion is covered by a 1-5 mm layer of connective tissue and mucous membrane (El-Shazly, 1991).
Monitoring included a 20-gauge intra-arterial catheter for direct blood pressure measurement. The haemodynamic goals were to maintain the Mean Arterial Pressure (MAP) at 55-60 mm Hg by adjusting the isoflurane concentration and the use of esmolol. The amount of blood loss, the consumption of isoflurane, frequency of use of esmolol were evaluated in both groups.
Extubation was performed after full recovery and awakening and ability of patients to follow verbal commands (eye opening or attempted self-extubation). The time interval between interruption of anesthetics and extubation was recorded as recovery time. A scoring system of postoperative respiratory system evaluation, named Postoperative Respiratory System Evaluation Scoring (PRSES), was formed for evaluation of postoperative respiratory complications (Kocamanoglu et al., 2006) (Table 1). PRSESs were noted at the 1st, 5th and 10th min after extubation by the same anesthetist.
| Table 1: | Postoperative Respiratory System Evaluation Scoring (PRSES) (Kocamanoglu et al., 2006) |
 | |
Complications such as headache, visual disturbances, postoperative nausea and vomiting (PONV), sore throat and swallow difficulty, which occurred in the operating room and Postanesthesia Care Unit (PACU), were recorded. In PACU also, Patients reporting pain score greater than 3 on VAS were managed with incremental intravenous doses of tramadol 10 mg. All patients also received 1 tablet of acetaminophen 300 mg at 1 h postoperatively. Pain scores and tramadol consumption were assessed every 15 min in PACU.
Statistical analysis: The Mann-Whitney u-test, independent t-test, x2 analysis or, Fisher's exact test were used as appropriate. A p-value of = 0.05 was considered statistically significant
RESULTS
Preoperative background of the patients did not significantly differ between the two groups (Table 2). All 30 patients completed the study. The operative time was comparable in the two groups. Blood loss in block group was significantly reduced in comparison to non-block group (70±3 mL vs 110±4 mL). No patient required blood transfusion or presented with excessive blood loss.
Intraoperatively, isoflurane consumption was less in block group than non-block one (p<0.001). All patients in the non-block group required supplemental esmolol to achieve the target MAP. In contrast, only 2 patients in the block group required supplemental esmolol (p<0.001). Recovery time was longer in non-block group than block group (Table 3).
PRSESs in all evaluation times were better in block group than non- block group. PRSESs were reclassified as PRSES-1 (no respiratory complication) and PRSES-2/5 (PRSES-2 + PRSES-3 + PRSES-4 + PRSES-5) (occurrence of a respiratory complication) in all groups for all evaluation times. The PRSES-1 was more frequent in block group than non-block group at all evaluation times after extubation (p<0.05) (Table 4).
VAS for pain was significantly lower in block group until 150 min (Fig. 3). In the PACU, the total tramadol consumption was 80.5 (3.3) and 30.2 (3.0) mg in non-block and block group respectively (p<0.01).
| Table 2: | Preoperative characteristics in both groups |
 | |
| Values are means (SD) except for sex and ASA | |
| Table 3: | Introperative and postoperative events and requirements in both groups |
 | |
| Table 4: | postoperative respiratory system evaluation scoring (PRSES) at 1st, fifth and 10th min after extubation (n, percentage of frequency) |
 | |
| *: p-value <0.001 | |
 | |
| Fig. 3: | The mean visual analog scale for pain scores in both groups; * p<0.05. 0 of x axis denoting the time of admission to PACU |
Other postoperative complications were more frequent in non-block group than block group at all evaluation times. Early postoperative complications except respiratory problems are shown in (Table 5). Failure rate was suspected in 2 cases.
| Table 5: | Early postoperative complications except respiratory problems and pain (n, percentage of frequency) |
 | |
| PONV: Postoperative nausea and vomiting | |
DISCUSSION
In the present study, the combined use of GA with Transnasal endoscopic SPGB in sinonasal surgery resulting in improved surgical field (decrease blood loss), reduction of medications used intraoperatively (isoflurane, esmolol), as well as postoperatively (tramadol), better recovery profiles (short recovery time), reduction of postoperative pain, reduction of postoperative respiratory complications (PRSESs 2-5 and others) and accepted surgeon and patient satisfaction.
Why we use the Transnasal Endoscopic technique? There are generally three approaches to block this ganglion; Sluder first advocated the sphenopalatine ganglion block transnasally with topical use of cocaine in 1908. Later, he advanced his technique to transnasal needle injection of carbolic acid (phenol) in an effort to obtain prolonged relief. Ruskin introduced the transoral and the lateral injection approaches thereafter (Yang and Oraee, 2006). The transnasal injection technique, either blindly or with the assistance of a speculum, carries the danger of nasal mucosa sloughing during needle insertion (Cambareri, 1997). This led to the development of the transnasal endoscopic technique in which the topical block, or needle infiltration, was performed under direct vision using angled rigid endoscope (Prasanna and Murthy, 1993). For the transoral approach, the identification of the needle entry point may be difficult in inexperienced hands. (Cambareri, 1997). The lateral infratemporal approach definitely requires image guidance (Cambareri, 1997; Day, 1999; Raj et al., 2003). The transnasal topical technique remains the most popular approach for the block because of its simplicity (Peterson et al., 1995; Saberski et al., 1999; Shah and Racz, 2004). It can be easily done with a cotton-tipped applicator soaked with local anesthetics or performed with local anesthetic dripping or spray (Russell, 1991). However, the diffusion of the topical anesthetics through the nasal mucosa is not predictable even with a properly placed applicator (Janzen and Scudds, 1997). Our method is under direct vision, accurate, safe needle injection technique. It is similar to the original transnasal topical approach but takes advantages of needle injection. No bleeding or other complications occurring after each block demonstrated its safety. Prolonged pain relief as compared with the results from topical technique (Redick, 1994) indicated its predictable and durable effect.
So, transnasal SPG injection via topically anesthetized nasal cavity, guided by endoscope, may be an effective alternative to the conventional techniques. The needle we used was a crude manual modification of an existing needle. A manufactured needle with a bent tip will better fit the variety in patient anatomy.
The use of endoscopy certainly facilitates the identification of the anatomic region corresponding to the pterygopalatine fossa, thus making it possible to inject the target site directly, although there are still a number of technical limitations preventing it: for example, some complex anatomic situations make it difficult or even impossible to enter the region of the sphenopalatine foramen. These limitations further explain some of the negative results and the fact that the treatment is clinically effective in some cases only after the use of repeated infiltrations (Felisati et al., 2006). This may explain the failure rate in our study (2 patients)
Why we use combined GA and RA in Sinonasal surgery?
| • | Why not RA alone? SPGB technique is simple and easy and is associated with fewer complications. This technique may be performed under GA, sedation, or alone. Sinonasal surgery may be performed under RA with sedation (Lee et al., 1997; Thaler et al., 1997), but the sinonasal surgery has increasingly been extended to involve deep sinus areas, such as the ethmoidal region. Such procedures cannot be performed under RA alone and GA is required (Jorisson et al., 1996). Thus it is safer to select GA combined with appropriate regional block than to select RA with heavy sedation in these cases. |
| • | Why not GA alone? There is evidence that the use of GA alone may be associated with excessive blood loss (Levine, 1990) 28). This observation is supported by the present study and other studies (Higashizawa and Koga, 2001; Stankiewics, 1989; Hoffman et al., 1990). The decreased blood loss and improved surgical field may be due to the analgesia developed secondary to local blockade. |
| • | Why combined? The use of regional blockade combined with GA over RA with sedation have many advantages including less patient discomfort, more airway security and more hemodynamic stability. In the present study the consumption of isoflurane and the need for esmolol were reduced significantly in block group. Also VAS pain scores and the need for tramadol postoperatively were reduced in the block group. These findings are in-line with Higashizawa and Koga (2001). |
What are the benefits from SPGB? Apart from all the above mentioned benefits as regard it is a local block, SPGB is considered one line of treatment and controlling chronic sinusitis; chronic sinusitis is often accompanied by the symptoms of postnasal drip, sinus fullness and pressure. There may be severe headache of the forehead (frontal), cheek (maxillary), eye (retro-orbital) and occipital areas of the head and neck. These headaches may be accompanied by nasal congestion with impaired nasal breathing; along with facial pain and tenderness; ear fullness, pain and ringing; and tooth and jaw discomfort. There may also be associated symptoms of breathing difficulty, including shortness of breath and wheezing.
The mucosal tissues lining the nose, nasopharynx and sinuses are stimulated by the sphenopalatine ganglia. These two ganglia supply the mucosa with sympathetic and parasympathetic nerve impulses. The sympathetic part causes vessel dilation and decreased mucous secretion. The parasympathetic part causes vessel constriction and increased mucous secretion. In chronic nasal congestion and sinusitis, there is an overabundance of parasympathetic nervous stimulation with persistent mucosal congestion. In long-standing sinusitis, an imbalance of the autonomic nervous system develops. Consequently, the patient experiences a vicious, perpetual cycle of continuous parasympathetic symptoms with a lack of sympathetic balance.
Anesthetizing these ganglia causes a temporary blocking of both sympathetic and parasympathetic nervous stimuli. This blockade resets the balance of both halves of the autonomic nervous system. The result is improvement of the symptoms of chronic sinusitis. There is decreased sinus pressure and headache, decreased facial pain and tenderness, improved sinus drainage, easier nasal breathing and improved vocal quality. Often ear ringing and jaw discomfort also improve (Milewski, 1996). This observation may explain the less PRSES 2-5 and other postoperative complications and better pain control in block group in our study.
In summary, the concomitant use of SPGB and general anesthesia was effective in patients undergoing sinonasal surgery. SPGB provided reduced isoflurane consumption, improved the surgical field (decreased blood loss), attenuated postoperative pain and reduced the postoperative tramadol requirement. In view of its effectiveness and relative safety, the SPGB may by used routinely as a supplement to GA in sinonasal surgery.
REFERENCES
- Felisati, G., F. Arnone, P. Lozza, L. Massimo, C. Marcella and B. Gennaro, 2006. Sphenopalatine endoscopic ganglion block: A revision of a traditional technique for cluster headache. Laryngoscope, 116: 1447-1450.
CrossRefDirect Link