
Dabiri Sh.
Department ofNuclear Medicine:
Tabriz University of Medical
Sciences,
Tabriz, Iran
Journal of Medical Sciences
Year: 2006 | Volume: 6 | Issue: 5 | Page No.: 806-811







ABSTRACT
Thyroid cancer is the most common endocrine malignancy. More than 90% of primary thyroid cancers are papillary or follicular types, together termed Differentiated Thyroid Cancers (DTC). The aim of this study was to assess to what extent 99mTc-MIBI Whole Body Scan (WBS) improves detectability of negative 131I scan in follow-up of patients with DTC. This descriptive and prospective study was performed over 40 patients with DTC who were referred to Dr. Dabiri Nuclear Medicine Center from 2004-2005. Six months after total thyroidectomy and 131I ablation therapy, all patients underwent 131I 99mTc-MIBI WBS. Serum thyroglobulin was measured by radioimmunoassay method. Serum TSH levels was >30 μU mL-1 in all patients. 99mTc-MIBI showed 93.75% sensitivity and 87.5% specificity. The figures for 131I scan were 87.5 and 100%, respectively. It is concluded that considering the slightly higher sensitivity of 99mTc-MIBI, this radio tracer can be used for follow-up of patients with negative 131I study and patients on suppression therapy.
PDF Abstract XML References Citation
How to cite this article
Dabiri Sh., 2006. 99mTc-MIBI Scintigraphy Versus 131I Whole Body Scan in the Follow-up of Patients with Differentiated Thyroid Carcinoma. Journal of Medical Sciences, 6: 806-811.
DOI: 10.3923/jms.2006.806.811
URL: https://scialert.net/abstract/?doi=jms.2006.806.811
DOI: 10.3923/jms.2006.806.811
URL: https://scialert.net/abstract/?doi=jms.2006.806.811
INTRODUCTION
Thyroid cancer is the most common (90%) endocrine malignancy. It constitutes 1.5% of all malignancies and is responsible for 0.04% of cancer related deaths (Sandler et al., 1996). More than 90% of primary thyroid cancers are papillary or follicular types. Papillary and follicular thyroid cancers, together termed Differentiated Thyroid Carcinoma (DTC), have an optimal prognosis (Eustatia-Rutten et al., 2006; Pagano et al., 2004; Mettler and Guiberteau, 1998). Most DTCs appear as asymptomatic thyroid nodules. Surgery is the primary treatment for thyroid cancers. Most clinicians recommend near-total or total thyroidectomy and then 131I ablation therapy, since its consequences are minimal and follow-up is facilitated. A Whole Body Scan (WBS) is performed 4 to 7 days after 131I treatment. Total thyroidectomy reduces the risk of recurrence and radioiodine ablation destroys any normal or neoplastic residuals of thyroid tissue. These procedures also improve the sensitivity of thyroglobulin (Tg) as a marker of disease and increase the sensitivity of 131I WBS for the detection of persistent or recurrent disease (Lupoli et al., 2005; Geus-Oei et al., 2002).
Because DTC may recur years after initial treatment, the follow-up of these patients is long-term (Schlumberger et al., 2004; Ali et al., 2001). The initial methods for the follow-up of DTC are measurement of serum Tg levels and Iodine-131 WBS which is performed after total thyroidectomy and Iodine-131 therapy (Sandler et al., 1996). Tg level is a specific and very sensitive marker of DTC recurrence. It is usually evaluated after eradication of thyroid residual tissue (by thyroidectomy and radioiodine therapy), in presence of high level of TSH (>35 μU mL-1) obtained with the suspension of therapy or after recombinant-TSH administration and in absence of anti-Tg antibodies. Recent advances in the follow-up of DTC are related to the use of recombinant human TSH (rhTSH) in order to stimulate Tg production and the ultrasensitive methods for Tg measurement. Undetectable serum Tg during TSH suppressive therapy with L-T4 does not exclude persistent disease, therefore serum Tg should be measured after TSH stimulation (Pagano et al., 2004; Lubin et al., 1994).
In patients with negative 13I WBS and high levels of Tg, one or more of the following investigations is considered: radiological examinations (neck US, skeletal X-ray, chest and abdominal CT, MRI) and scintigraphy (bone scintigraphy, 99mTc-MIBI or Tl-201 scintigraphy, Octreoscan, PET/CT). The use of PET is well known in patients in whose metastases are strongly suspected and who are unable of concentrating 131I. Considering the hypothesis of a recurrence with lesion size below the resolution power of the diagnostic equipment (5 mm), if PET/CT results are negative, the patients are strictly followed-up and Tg is monitored every 4-6 months (Biscontini et al., 2004).
Tl-201 scintigraphy and 99mTc MIBI imaging are two alternative methods to 131I WBS for the follow-up of patients with DTC (Sriprapaporn et al., 2002; Braverman and Utiger, 2000). MIBI scan combined with neck US could be proposed as a first-line diagnostic imaging modality in the follow-up of DTC patients with elevated serum Tg levels and negative 131I scan (Casara et al., 1999; Gallowitsch et al., 1998).
In the case of high levels of Tg and negative 131I, Tl-201 and 99mTc MIBI scintigraphy are better (Lin et al., 1998). More than 50% of cases for which 131I was normal are positive for Tl-201 and 99mTc- MIBI (Fujie et al., 2005). On the other hand, the iodine WBS is uncomfortable because of the need for discontinuation of thyroid hormone therapy and repeated visits for facilitating the nuclear medicine therapy.
The aim of this study was to compare the capabilities of former methods of differentiated thyroid cancer follow-up (131I scan and Tg measurement) with an alternative method, 99mTc-MIBI scintigraphy. If the sensitivity of 99mTc-MIBI scintigraphy be similar with former methods, then discontinuation of medical therapy and induction of hypothyroidism for 131I scan will not be required.
MATERIALS AND METHODS
This is a descriptive and prospective study performed over 40 patients with differentiated thyroid cancer who were referred to Dr. Dabiri Nuclear Medicine Center from 2004-2005. The patients were selected randomly and (after achievement of informed consent). There were no certain inclusion criteria in this study or sex and age limitation for sampling. Six months after total thyroidectomy and 131I ablation therapy, all patients underwent 131I and 99mTc-MIBI WBS and measurement of serum Tg levels.
Because of no administration of hormone therapy, serum TSH levels in all patients was >30 μU mL-1, which is required for maximizing Tg secretion by residual and metastatic tissue as well as for maximum 131I absorption.
At first serum thyroglobulin was measured by radioimmunoassay method. The levels ≥2 ng dL-1 and <2 mg dL-1 were considered positive and negative, respectively. Then, 48-72 h after oral administration of 3 mci of 131I the patients underwent posterior and anterior whole-body scanning. Planar images were obtained by means of Siemens Orbiter Gamma Camera with a high-energy parallel hole collimator having capability to collect 300 000 counts in each view. We performed 99mTc-MIBI WBS following IV injection of 15 mci of 99mTc-MIBI one week before 131I WBS. The posterior and anterior images were obtained by means of a n ADAC Dual-head Gamma Camera fitted with a low-energy parallel hole collimator. All images were interpreted by one nuclear medicine specialist considering criteria as following: 131I is concentrated normally in some extra-thyroid areas. It is absorbed by salivary and gastric glands and then is secreted into mouth and stomach and can be found in esophagus. So, in the cases of detection of mediastinal uptake, scanning was repeated after ingestion of some water. The iodine is also secreted into urine and it is normally visible in bladder and colon. The liver is reservoir of thyroid hormones; so, radioactivity uptake in liver is normal, whereas obvious focal uptake is indicative of metastatic lesion. Focal radioactivity uptake is also seen in other metastatic regions including cervical and Para-tracheal lymph nodes.
The interpretation of radioactive agent absorption in thyroid bed was done according to the extension of primary cancer. If there was no evidence of cancer aggression or non-complete tumor resection in pathology, the radioactivity was considered normal, whereas radioactivity in presence of tumor penetration to thyroid capsule or tumor extension beyond to 2 mm of resection margin (according to pathology results) was considered as cancer remnant.
Finally, the achieved data were analyzed by SPSS-12 statistical software. Chi-square test was used for determination of significance of relations and differences between results; and p-value less than 0.05 was considered statistically significant.
RESULTS
This study was performed over 40 patients with differentiated thyroid cancer. Their ages ranged from 23 to 63 years, with an average of 43.5 years. Of all patients 36 cases had papillary cancer and 4 cases had follicular cancer of thyroid. The average ages of patients with papillary and follicular cancer were 43.75 and 41.75 years, respectively. Of patients with papillary cancer, 22.2% were male and 77.8% were female, whereas male to female ratio in patients with follicular cancer was 1.
Of all patients 24 cases (60%) had TG level of less than 2 ng dL-1 (negative result) and 16 cases (40%) had TG level of ≥2 ng dL-1 (positive result).
The result of 131I scan was negative in 26 cases (65%) and was positive in 14 cases (35%, Fig. 1). All positive scans had neck uptakes.
 | |
| Fig. 1: | Lymph node metastasis in WBS with 131I |
| Table 1: | The comparisons of results of 131I scan with Tg levels |
 | |
| Table 2: | The comparisons of results of Tc-MIBI scan with Tg levels |
 | |
| Table 3: | The comparisons of results of 131I with 99mTc-MIBI scan |
 | |
Table 1 shows the comparison of results of I-131 scan with Tg levels.
The result of 99mTc-MIBI scan was negative in 22 cases (55%) and was positive in 18 cases (45%, Fig. 2). 99mTc-MIBI uptake was observed in neck and axillary region. Table 2 shows the comparison of result of 99mTc-MIBI scan with Tg levels. Three patients had positive 99mTc-MIBI scan whereas their serum Tg was at negative level. According to the false/true positive and false/true negative results the sensitivity and specificity of 131I scan were calculated as 87.5 and 100%, respectively. Also, the 99mTc-MIBI scan had the sensitivity of 93.75% and specificity of 87.5%. Table 3 shows the comparison of results of WBS with 99mTc-MIBI and I-131. Regarding the slightly higher sensitivity of 99mTc-MIBI scan, it can be used for follow-up of patients with DTC.
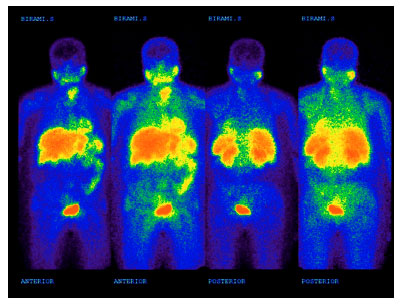 | |
| Fig. 2: | Local metastases in 99mTc-MIBI WBS of patient with papillary carcinoma |
DISCUSSION
Papillary carcinomas are the most common thyroid malignancies (Hsu et al., 2003). The ratio of patients with papillary or follicular type of DTCs in present study was 9 to 1 which is compatible with references (Sandler et al., 1996). In present study, the average ages of patients with papillary and follicular carcinoma of thyroid were 43.75 and 41.75 years, respectively. Regarding to the reported average ages of 45 years for papillary and 53 years for follicular carcinoma in references (Sandler et al., 1996), it appears that the average age of patients with papillary carcinoma is compatible with references but that of patients with follicular carcinoma is lower. This difference is attenuated by the fact that there were only 4 cases of follicular carcinoma, of which 3 had the ages of less than 50.
The female to male ratio of patients with papillary carcinoma in present study was 3.5 to 1, which is more than 2 to 1 ratio reported in the references (Sandler et al., 1996). This may be due to the fact that in spite of randomized selection of the patients, majority of our cases (75%) were female. The male to female ratio in patients with follicular carcinoma was 1 and according to the Chi-square test, there was no significant relation between the age of patients and the type of cancer (PV = 0.25).
Tg levels were measured under endogenous thyroid-stimulating hormone stimulation after withdrawal of L-thyroxin treatment (off-T4), has been proven to be the most sensitive method for evaluation of patients with recurrent malignancy or distant metastases (Cailleux et al., 2000; Gallowitsch et al., 1998). One study used a comparative approach between low-dose 131I scan and the 99mTc-tetrofosmin whole-body scintigraphy and concluded that scintigraphy with 99mTc-tetrofosmin has clear advantages concerning sensitivity in most metastatic lesions when compared with low-dose 131I scan. Despite a slight lower specificity, 99mTc-tetrofosmin WBS has been proven to be a useful tool in the assessment of metastatic lesions in differentiated thyroid carcinoma (Gallowitsch et al., 1998).
A study by Hahnemann University (Philadelphia) showed that 99mTc-MIBI is a suitable alternative to 201Tl scintigraphy in thyroid carcinoma, especially following thyroidectomy and 131I therapy. 131I scintigraphy with serum Tg is adequate in both pre- and post-ablation patients. Among the post-131I ablation patients, 99mTc-MIBI or 201Tl is extremely valuable for tumor localization, especially when the 131I WBS is negative. The combination of 99mTc-MIBI or 201Tl scintigraphy with 131I and serum Tg offers the highest diagnostic yield (Dadparvar et al., 1995).
A retrospective study in University of Sapienza (Rome, Italy) over patients with metastases from DTC, evaluated the results of 131I WBS in 269 patients (performed 40 days after surgery) and also the result of first Tg measurement in 69 of them (performed the day before the whole-body scan). In more than 80% of patients, metastases were suspected or diagnosed as early as 40 days after surgery in the presence of residual thyroid tissue by combined evaluation of results of WBS and Tg measurement. Also, WBS detected distant metastases more frequently than local lymph node metastases (Filesi et al., 1998).
Another study showed that 99mTc MIBI SPECT is a useful tool to detect metastatic lesions in PTC with elevated Tg but negative 131I WBS. However, although 99mTc- MIBI SPECT is a more accurate method for detecting the local lymph node metastases, small lymph node and lung metastases may be missed in this scan (Hsu et al., 2003).
In this study, we did not determine the sensitivity of 131I and 99mTc-MIBI scans separately for distant and local metastases, because there was no case of distant metastasis in our patients. We didn’t perform neck sonography, because we were looking for distant metastases, too. According to the results obtained in this study, the sensitivity of 99mTC-MIBI scan was 93.75% which is higher than the results obtained in other studies. It was probably because of low level of false-negative cases.
Also, the specificity of 99mTc-MIBI scan was 87.5% which is lower than the results reported by other studies. This is because of the fact that 2 of 3 false-positive cases obtained in 99mTc-MIBI scan were axillary lymph nodes uptake which seems to be due to the inflamated lymph nodes (Elser et al., 1997).
Rubello et al. (2000) showed that regarding distant metastases, MIBI scan provided results similar to those of conventional imaging (CT, MRI, 99mTc-methylene diphosphonate bone scan). However, it had 100% specificity in contrast to low sensitivity (46.15%) in detecting thyroid remnants.
Another study in Siriraj Hospital to evaluate the potential of 99mTc-MIBI imaging for the follow-up of patients with DTC showed 72% sensitivity (Sriprapaporn et al., 2002).
In a study performed in Nuclear Medicine Department of Kyoto University (Japan) over 68 thyroidectomized thyroid cancer patients, the detection sensitivity of 99mTc-MIBI was 94.4% for neck, 78.4% for lung and 92.8% for skeletal lesions; This study reveals that 99mTc-MIBI can be proposed as a first-line diagnostic agent for the follow-up protocol of thyroid cancer patients, although the ability to detect small lung metastases is somewhat limited (Alam et al., 1998).
A study was performed in Radiology Department of Miyazaki Medical College to compare the capability of 99mTc-MIBI, 131I and 201Tl to detection of metastasis in DTC. Forty patients after total thyroidectomy were evaluated. This study concluded that both 99mTc-MIBI and 201Tl should be used in cases with high serum Tg even with negative 131I uptake. Based on the fact there was no prominent difference between 99mTc-MIBI and 201Tl in the detectability of metastasis, 99mTc-MIBI might be more suitable tracer because of better quality image (Nagamachi et al., 2000).
A study in Brazil Federal University Division of Nuclear Medicine (Almeida-Filho et al., 2000) evaluated 99 patients with DTC who had total or nearly total thyroidectomy. It showed that 99mTc-MIBI and Tg results were in agreement in 96%. 99mTc-MIBI scan can show the sites of tumoral activity with optimal image resolution, particularly in those with abnormal Tg and negative 131I WBS results. 131I WBS in patients having ablation should be reserved only for therapy planning.
A study in Radiology Department of Okayama University (Japan) investigated the diagnostic capabilities of 131I, Tl-201 and Tc-99m-MIBI scintigraphy for thyroid cancer metastases after total thyroidectomy over the entire body and for every locus before and after thyroid bed ablation (Fujie et al., 2005). This study was performed over 36 cases of thyroid cancer and suggested that for whole-body sensitivity, both Tl-201 and 99mTc-MIBI were high before ablation and 131I was high after ablation.
The sensitivity of 131I scan was 87.5% which is higher than the results reported by some other studies. Also, the specificity of 131I scan was 100% which is compatible with the results reported by other studies.
In the study by Sriprapaporn et al. (2002), 99mTc MIBI showed 72% sensitivity, 100% specificity and 77% accuracy. The figures for 131I scan were 57, 100 and 66%, respectively.
CONCLUSIONS
Regarding to the higher sensitivity of 99mTc MIBI scintigraphy in comparison to 131I WBS in this study, and no requirement for withdrawal of L-thyroxin treatment (off-T4) in order to perform 99mTc-MIBI scan, this modality can be used as an alternative method for follow-up of patients with metastatic DTC after total thyroidectomy and hormone therapy.
REFERENCES
- Ali, S., B. Siema, A.M. Majid, A.H. Alya, A. Abdulraouf and A.H. Abdallah, 2001. 123I isotope as a diagnostic agent in the follow-up of patients with differentiated thyroid cancer: Comparison with post 131I therapy whole body scanning. J. Clin. Endocrinol. Metabol., 86: 5294-5300.
Direct Link - Almeida-Filho, P., G.C. Ravizzini, C. Almeida, S. Borges-Neto, 2000. Whole-body Tc-99m sestamibi scintigraphy in the follow-up of differentiated thyroid carcinoma. Clin. Nucl. Med., 25: 443-446.
Direct Link - Biscontini, G., M. Possa, R. Sara, M. Milella and C. Rossetti, 2004. Diagnostic modalities in patients affected by differentiated thyroid carcinoma with high thyroglobulin levels and total body Iodine-131 negative: PET/CT use after rec. TSH. Minerva Endocrinol., 29: 151-160.
Direct Link - Cailleux, A.F., E. Baudin, J.P. Travagli, M. Ricard and M. Schlumberger, 2000. Is diagnostic iodine-131 scanning useful after total thyroid ablation for differentiated thyroid cancer? J. Clin. Endocrinol. Metab., 85: 175-178.
Direct Link - Casara, D., D. Rubello, G. Saladini, R. Mazzarotto, G. Sotti, G. Tomasella and M.R. Pelizzo, 1999. Clinical approach in patients with metastatic differentiated thyroid carcinoma and negative 131I whole body scintigraphy: Importance of 99mTc MIBI scan combined with high resolution neck ultrasonography. Tumori, 85: 122-127.
- Dadparvar, S., A. Chevres, M. Tulchinsky, L. Krishna-Badrinath, A.S. Khan and W.J. Slizofski, 1995. Clinical utility of technetium-99m methoxyisobutylisonitrile imaging in differentiated thyroid carcinoma: Comparison with thallium-201 and iodine-131 Na scintigraphy and serum thyroglobulin quantitation. Eur. J. Nucl. Med., 22: 1330-1338.
- Eustatia-Rutten, C.F., E.P. Corssmit, N.R. Biermasz, A.M. Pereira, J.A. Romijn and J.W. Smit, 2006. Survival and death causes in differentiated thyroid Carcinoma. J. Clin. Endocrinol. Metab., 91: 313-319.
Direct Link - Fujie, S., Y. Okumura, S. Sato, S. Akaki, K. Katsui, K. Himei, M. Takemoto and S. Kanazawa, 2005. Diagnostic capabilities of I-131, TI-201 and Tc-99m-MIBI scintigraphy for metastatic differentiated thyroid carcinoma after total thyroidectomy. Acta. Med. Okayama, 59: 99-107.
Direct Link - Geus-Oei, L.F., H.Y. Oei, G. Hennemann and E.P. Krenning, 2002. Sensitivity of 123I whole-body scan and thyroglobulin in the detection of metastases or recurrent differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imag., 29: 768-774.
Direct Link - Hsu, C.H., F.Y. Liu, R.F. Yen and C.H. Kao, 2003. Tc-99m MIBI SPECT in detecting metastatic papillary thyroid carcinoma in patients with elevated human serum thyroglobulin levels but negative I-131 whole body scan. Endocrine Res., 29: 9-15.
Direct Link - Lupoli, G.A., F. Fonderico, S. Colarusso, A. Panico and A. Cavallo et al., 2005. Current management of differentiated thyroid carcinoma. Med. Sci. Monit., 24: RA368-RA373.
Direct Link - Nagamachi, S., S. Jinnouchi, R. Nishii, H. Nakahara and S. Futami et al., 2000. Evaluation of technetium-99m-MIBI scintigraphy in metastatic differentiated thyroid cancer: Comparison study with 131I and 201Tl. Jap. J. Nucl. Med., 37: 89-98.
Direct Link - Pagano, L., M. Klain, M. Pulcrano, G. Angellotti and F. Pasano et al., 2004. Follow-up of differentiated thyroid carcinoma. Minerva Endocrinol., 29: 161-174.
Direct Link - Rubello, D., R. Mazzarotto and D. Casara, 2000. The role of technetium-99m methoxyisobutylisonitrile scintigraphy in the planning of therapy and follow-up of patients with differentiated thyroid carcinoma after surgery. Eur. J. Nucl. Med., 27: 431-440.
Direct Link - Schlumberger, M., G. Berg, O. Cohen, L. Duntas and F. Jamar et al., 2004. Follow-up of low-risk patients with differentiated thyroid carcinoma: A European perspective. Eur. J. Endocrinol., 150: 105-112.
Direct Link - Sriprapaporn, J., C. Toopmongkol, B. Satayaban and N. Chantamoon, 2002. Technetium-99m methoxyisobutylisonitrile imaging in the follow-up of differentiated thyroid carcinoma. Ann. Acad. Med. Singapore, 31: 195-198.
Direct Link