
K. Philip
Division of Microbiology, Institute of Biological Sciences, Faculty of Science, University of Malaya, Kuala Lumpur, Malaysia
W.Y. Teoh
Division of Microbiology, Institute of Biological Sciences, Faculty of Science, University of Malaya, Kuala Lumpur, Malaysia
S. Muniandy
Department of Molecular Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
H. Yaakob
Department of Oral Pathology, Oral Medicine and Periodontology, Faculty of Dentistry, University of Malaya, Kuala Lumpur, Malaysia
Journal of Biological Sciences
Year: 2009 | Volume: 9 | Issue: 5 | Page No.: 438-444







ABSTRACT
This study identifies the major pathogens that constitute the normal oral flora of Malaysians and elaborates on their pathogenic potential. Major oral microorganisms identified by their 16S rDNA sequences include Streptococcus pneumoniae, Staphylococcus aureas, Streptococcus mitis and Neisseria subflava in the gingival crevice, Streptococcus oralis, Rothia mucilaginosa and Kingella oralis on teeth surface, Streptococcus infantis, Streptococcus pseudopneumoniae, Actinomyces viscosus on tongue surface. Organisms identified non-pathogenic included Pseudomonas aeruginosa in the gingival crevice, Streptocccus sanguis on teeth surface and Lautropia sp. on tongue surface. The presence of pathogenic organisms may have profound implications on the health of individuals harbouring them. Knowledge of the type of bacteria that inhabit the oral cavity is important in predicting and preventing not only dental diseases but also the associated systemic complications caused by them.
PDF Abstract XML References Citation
How to cite this article
K. Philip, W.Y. Teoh, S. Muniandy and H. Yaakob, 2009. Pathogenic Bacteria Predominate in the Oral Cavity of Malaysian Subjects. Journal of Biological Sciences, 9: 438-444.
DOI: 10.3923/jbs.2009.438.444
URL: https://scialert.net/abstract/?doi=jbs.2009.438.444
DOI: 10.3923/jbs.2009.438.444
URL: https://scialert.net/abstract/?doi=jbs.2009.438.444
INTRODUCTION
Approximately seven hundred microbial species in the biofilm of the oral cavity are nourished with nutrients and provided with a conducive habitat. In addition, the dental plaque provides a cocoon for them, while the dextran they secrete allow them to bind to tooth surfaces. In species like Strep. mitis and Strep. sanguis combined there is good correlation between in vitro binding properties and cariogenicity (Willcox et al., 1985). The non-shedding tooth surface also provides for development of a complex ecosystem in the mouth.
In the oral cavity, the bacterial population is a result of the dynamic relationship between pathogens and commensals (Socransky et al., 2002). In the last decade, it has become increasingly clear that oral diseases, especially periodontitis are associated with and independent risk factors for systemic conditions such as cardiovascular disease, osteoporosis, diabetes mellitus and infection in other body sites (Renvert, 2003; Meurmann et al., 2004).
Commensal microorganisms found in the oral cavity rarely cause invasive infections except in immunocompromised adults or children. However, non beneficial microorganisms have direct link to dental caries, periodontal disease and halitosis. In immunocompromised hosts however, these microorganisms can cause opportunistic infections and systemic diseases. Oral bacteria have been implicated in bacterial endocarditis, aspiration pneumonia, osteomyelitis in children, preterm low birth weight, coronary heart disease and cerebral infarction (or stroke). The incidence of bacteremia following dental procedures has been well documented (Li et al., 2000). The major oral diseases are caused by disruption of homeostasis in the polymicrobial activity.
The type and distribution of oral microorganism in the biofilm vary with dietary and cultural habits and the health of individuals (Bowden and Li, 1997). A good understanding of the types and characteristics of the microbes of the oral cavity would be useful in managing infections caused by them. Knowledge of the susceptibility or resistance of these species to specific antibiotics will enhance therapeutic efficacy.
MATERIALS AND METHODS
This study was conducted between December 2007 and November 2008 in the Faculty of Science and Medicine of the University of Malaya.
Sample collection: Bacterial species were identified by their 16S rDNA sequences. Bacteria were collected using either the Gracey curette (teeth surface and gingival crevice) or cotton swab (tongue). Swabbed samples were suspended in Reduced Transport Fluid (RTF) and diluted 10, 102 and 103 times. Diluted samples were plated in duplicate on Columbia blood agar plates and incubated aerobically at 37°C for 3-5 days. Distinct colonies (2-3 colonies of apparently same morphology) were selected and streaked separately on agar plates. Single colonies obtained were characterized by gross (colour and shape) and microscopic morphology as well as by gram staining.
DNA preparation: The genomic DNA of pure cultures was prepared using i-genomic DNA extraction mini kit (iNtRON Biotechnology, Seongnam). Extracted DNA was evaluated for both quality and quantity by agarose gel (1%) electrophoresis.
PCR and sequencing: Universal primers for 16S rDNA (forward: 5’-AGA GTT TGA TCA TGG CTC AG and reverse: 5’-TAC GGC TAC CTT GTT ACG ACTT) were used for PCR amplification. PCR conditions were: initial denaturation at 94°C for 5 min, denaturation at 94°C for 1 min, annealing at 52°C for 1 min, extension at 72°C for 1.5 min and final extension at 72°C for 10 min. PCR reaction mixtures (20 μL total) contained 2 μL of 10x PCR buffer, 2 μL of dNTP mix (2.5 mM each), 1 μL of each primer (10 pmoles), 50 ng of DNA template, 0.5 μL of i-TaqTM DNA polymerase 5U μL, iNtRON Biotechnology, Seongnam). The resulting PCR product was examined by electrophoresis on a 1.5% agarose gel and purified by PCR Quickspin kit (iNtRON Biotechnology, Seongnam). DNA sequencing of the PCR product was performed by Macrogen, Seoul.
Species identification: Sequences were blasted to NCBI databases using BlastN and bacterial species identified on the basis of at least 98% similarity to database 16S RNA sequences. Cross reference was also made to the Human Oral Microbiome Database (HOMD) at http://www.homd.org.
RESULTS
Table 1 shows the percentage homology of the 16S rDNA sequences with NCBI Genbank sequence data. Species identity was established on the basis on at least 98% homology.
Accession numbers shown in the first column represent those allocated for our sequences, while those shown in the last column are sequences deposited in the Genbank.
| Table 1: | Accession number and homology with Genbank sequences |
 | |
 | |
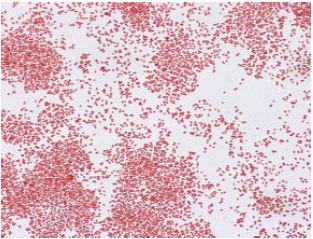
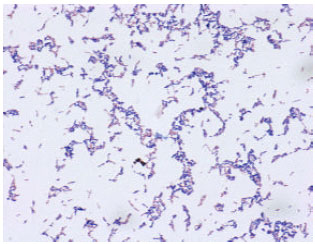
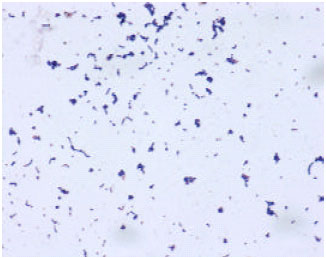
| Fig. 1: | Gram stain showing characteristics of Streptococcus pneumoniae |
Pathogenic organisms
Gingival crevice: Streptococcus pneumoniae (Fig. 1), an alpha hemolytic and gram positive diplococcus is a inhabitant of the upper respiratory tract that can cause a number of life threatening diseases. Streptococcus pneumoniae is the main respiratory tract pathogen in otitis, sinusitis, bronchitis, meningitis, bacteraemia and community acquired pneumonia. Clinical infections with pneumoniae have been managed with antibiotic and vaccines although antibiotic resistant strains are common and many distinct serotypes exist. The bacteria have been found to have resistance to β-lactams, macrolides and fluoroquinolones (Pallares, 2003; Rossoni et al., 2008). Mutation at pneumolysin (Ply), Pneumococcal surface protein A (PspA) and Pneumococcal surface protein C (PspC) which are important for the colonization of the respiratory tract did not prevent the animal model from infection.
 | |
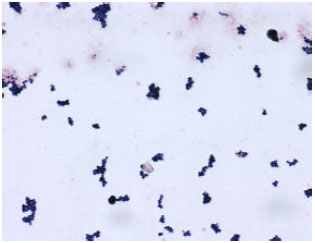
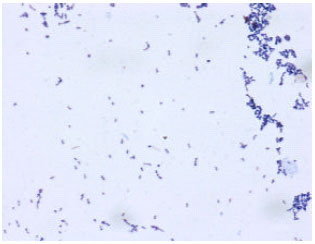
| Fig. 2: | Gram stain showing characteristics of Staphylococcus aureus |
 | |
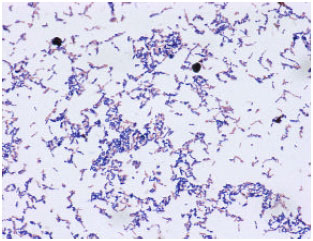
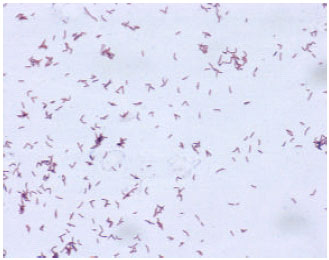
| Fig. 3: | Gram stain showing characteristics of Streptococcus mitis |
This study demonstrated that pneumococcal pathogenesis is complex and multifactorial (Ogunniyi et al., 2007). Mutants defective in growth rate remained capable of causing disease in animals as tested in mice and this study also showed that the pathogenesis is complex (Fernebro et al., 2008).
Staphylococcus aureus (Fig. 2) are gram positive cocci as well as coagulase positive. Methycillin Resistant Staphylococcus Aureus (MRSA) are commonly found pathogens (Gould, 2007). Streptococcus aureus is frequently reported as a pathogen causing nosocomial infections, bacteraemia and endocarditis (Gould, 2007; Fowler et al., 2006). Frequent antibiotic administration can lead to selection of resistant strains over susceptible strains (Schentag et al., 1998).
Streptococcus mitis (Fig. 3) can be an important pathogen in adults and may cause infections including endocarditis and toxic shock-like syndrome.
 | |
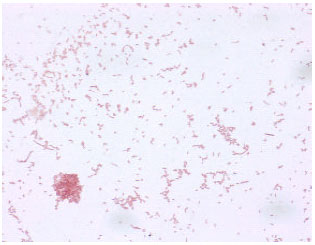
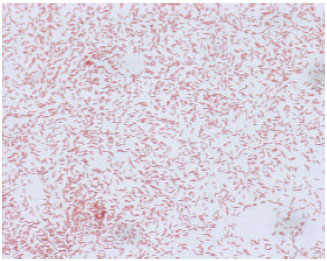
| Fig. 4: | Gram stain showing characteristics of Neisseria subflava |
 | |
| Fig. 5: | Gram stain showing characteristics of Streptococcus oralis |
Neisseria subflava (Fig. 4), a gram negative diplococcus may cause individuals to become susceptible to Streptococcal throat infections due to commensalism. In rare conditions it may cause Continuous Ambulatory Peritoneal Dialysis (CAPD) related peritonitis. This organism has also been implicated in meningitis, septicemia, endocarditis and endophthalmitis. The emergence of N. subflava isolates resistant to penicillin, fluoroquinolones and tetracycline have been noticed (Furuya et al., 2007). In response to ingested ethanol, Neisseria in the oral cavity could produce significant amount of carcinogenic acetaldehyde which is the risk factor for cancer of the upper aerodigestive tract (Muto et al., 2000).
Teeth surface: Streptococcus oralis (Fig. 5) are gram positive coccoid bacteria implicated in endocarditis.
 | |
| Fig. 6: | Gram stain showing characteristics of Rothia mucilaginosa |
 | |
| Fig. 7: | Gram stain showing characteristics of Kingella oralis |
Rothia mucilaginosa (Fig. 6) are normal oral flora which are catalase negative gram positive cocci. In rare cases it may cause bacterial meningitis and bacteremia. It has been reported that R. mucilaginosa cause late prosthetic joint infection and antibiotic prophylaxis is used for infection prevention of joint arthroplasties during dental procedures.
Kingella oralis (Fig. 7) gram negative rods or coccobacilli has been isolated from human dental plaque and may be associated with periodontis.
Tongue surface: Streptococcus infantis (Fig. 8) is an alpha hemolytic gram positive pathogen of the oral cavity.
Streptococcus pseudopneumoniae (Fig. 9) is genetically distinct from S. pneumoniae and is associated with Chronic Obstructive Pulmonary Disease (COPD). It is a non capsulated alpha hemolytic gram positive organism.
 | |
| Fig. 8: | Gram stain showing characteristics of Streptococcus infantis |
 | |
| Fig. 9: | Gram stain showing characteristics of Streptococcus pseudopneumoniae |
Actinomyces viscosus (Fig. 10) is gram positive filamentous bacteria occuring in dental plaque on cementum. In rare cases, this has been implicated in causing endocarditis.
Non-pathogenic organisms
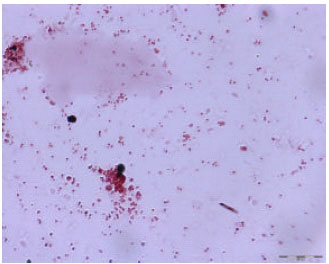
Gingival crevice: Pseudomonas aeruginosa (Fig. 11), a gram negative aerobic rod shaped bacteria is found in the environment. Antibiotic resistance in this species is common.
Teeth surface: Streptococcus sanguis (Fig. 12) is associated with good oral health and lack of this organism indicates caries susceptibility. Streptococcus sanguinis has been implicated in native-valve infective endocarditis and bacteremia. These infections may be complicated by the increase of antibiotic resistance (Xu et al., 2007).
 | |
| Fig. 10: | Gram stain showing characteristics of Actinomyces viscosus |
 | |
| Fig. 11: | Gram stain showing characteristics of Pseudomonas aeruginosa |
 | |
| Fig. 12: | Gram stain showing characteristics of Streptococcus sanguis |
 | |
| Fig. 13: | Gram stain showing characteristics of Lautropia |
Tongue surface: Lautropia sp. (Fig. 13) notably mirabilis are commonly found in the oral cavity and are gram negative cocci (Rossmann et al., 1998).
DISCUSSION
The development of the oral microbial community involves competition as well as synergy among the hundreds of species present in the oral cavity. Bacterial populations in the human oral cavity are constantly in a dynamic state of change. The need to profile and characterize these microorganisms using appropriate rapid detection methods can go a long way in developing future management strategies in clinical settings to enhance oral health in the Malaysian population.
Traditional methods for bacterial identification depended on phenotypic analyses which by themselves can cause misidentification of strains. Misidentification is usually either due to not all members of a given species may be positive for a particular identifying trait (Beighton et al., 1991; Kilian et al., 1989) or strains undergoing phenotypic shifts (Hillman et al., 1989; Tardiff et al., 1989). Due to its specificity and sensitivity, PCR based methods are currently widely applied for diagnostic purposes. Since 16S rDNA occur in multiple copies in the bacterial cell, it is a ideal target for taxonomic purposes. Additional targets such as 16S-23S rRNA intergenic spacer genes and species-specific virulence factors have provided some degree of specificity (Hoshino et al., 2005).
Streptococci are the predominant bacterial organisms in the human oral cavity. In general, oral streptococci can be divided into six distinct groups: Strep. gordonii, Strep. sanguis, Strep. oralis, Strep. mitis, Strep. parasanguis and Strept. crista (Rudney and Larson, 1993; Coykendall, 1989). Many species of this gram positive coccus are found in the oral cavity of Malaysian subjects. These include Strep.pneumoniae, Strep. pseudopneumonia, Strep. mitis, Strep. infantis, Strep. oralis. Non streptococci include Staphylococcus aureus, Neisseria subflava, Rothia mucilaginosa, Kingella oralis and Actinomyces viscosus. All of them may be considered important oral or systemic pathogens.
The occurrence of opportunistic pathogens in the oral cavity may be seen from the following aspects:
| • | Oral hygiene: Good oral hygiene would presumably allow the oral cavity to be colonized by a larger number of beneficial organisms and lower the number of pathogenic strains. Treatment by reduction of bacterial populations by antimicrobial or mechanical means is usually unsuccessful because the target bacteria are able to rapidly repopulate the oral cavity immediately after treatment (Burton et al., 2005) |
| • | Dental treatment procedures that introduce oral bacteria into the bloodstream: It has been established that oral bacteria are found in blood following dental procedures (Bahrani-Mougeot et al., 2008) and the American Heart Association has issued guidelines and updates on procedures to prevent bacterial endocarditis (Wilson et al., 2007) |
| • | Probiotics: The use of probiotics offer oral benefits (Caglar et al., 2005). One strategy employed is the depletion of oral bacteria by use of the antimicrobial chlorhexidine and repopulation of the oral cavity with beneficial organisms such as S. salivarius, a benign commensal probiotic (Burton et al., 2005) |
| • | Clinical management of oral cavity and systemic infections: Li et al. (2000) have evaluated the status of oral infections as a causal factor for systemic diseases and have discussed mechanisms or links between oral infection and secondary systemic effects. Since both gram positive and gram negative bacteria can potentially cause systemic infections, any management strategy must take this into account. Furthermore, many bacteria are antibiotic resistant or have the potential to acquire resistance. The relationship between oral health and general health is bidirectional and complex (Johnson et al., 2006). Brook (2003) describes the prudent management of odontogenic infection and preventive strategies in a comprehensive article |
The oral cavity of Malaysian subjects also contains non pathogenic bacteria including Capnocytophaga granulosa, Strep. sanguis and Lautropia. These organisms are important in maintaining the proper ecology of the oral cavity. This may in part help to maintain good oral health.
CONCLUSION
The large number of pathogenic bacterial species present in the oral cavity of Malaysian subjects may indicate that the potential for the development of systemic diseases is always present. The non-pathogenic bacteria may be beneficial in maintaining the balance of species in the oral cavity.
REFERENCES
- Bahrani-Mougeot, F.K., B.J. Paster, S. Coleman, J. Ashar, S. Barbuto and P.B. Lockhart, 2008. Diverse and novel oral bacterial species in blood following dental procedures. J. Clin. Microbiol., 46: 2129-2132.
Direct Link - Beighton, D., J.M. Handle and R.A. Whiley, 1991. A scheme for the identification of viridans streptococci. J. Med. Microbiol., 35: 367-372.
Direct Link - Bowden, G.H.W. and Y.H. Li, 1997. Nutritional influences on biofilm development. Adv. Dent. Res., 11: 81-99.
CrossRefDirect Link - Burton, J. P., C.N. Chilcott and J.R. Tagg, 2005. The rationale and potential for the reduction of by oral malodour using Streptococcus salivarius probiotics. Oral Dis., 11: 29-31.
CrossRef - Caglar, E., B. Kargul and I. Tanboga, 2005. Bacteriotherapy and probiotics role on oral health. Oral Dis., 11: 131-137.
CrossRef - Coykendall, A.L., 1989. Classification and Identification of the viridans streptococci. Clin. Microbiol. Rev., 2: 315-328.
Direct Link - Rossoni, A.M.O., L.M.D. Costa, D.B. Berto, S.S. Farah, M. Gelain and M.C.D.C. Brandileone et al., 2008. Acute bacterial meningitis caused by Streptococcus pneumoniae resistant to the antimicrobian agents and their serotypes. Arq. Neuro-Psiquiatr., 66: 509-515.
CrossRefPubMedDirect Link - Fernebro, J., C. Blomberg, E. Morfeldt, H. Wolf-Watz, S. Normark and B.H. Normark, 2008. The influence of in vitro fitness defects on pneumococcal ability to colonize and to cause invasive disease. BMC Microbiol., 8: 65-76.
Direct Link - Fowler, Jr. V.G., H.W. Boucher, G.R. Corey, E. Abrutyn and A.W. Karchmer et al., 2006. Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus. Neng. J. Med., 355: 653-665.
Direct Link - Furuya, R., Y. Onoye, A. Kanayama, T. Saika, T. Iyoda, M. Tatewaki and K. Matsuzaki, 2007. Antimicrobial resistance in clinical isolates of Neisseria subflava from the oral cavities of a Japanese population. J. Infection Chemoth., 13: 302-304.
Direct Link - Hillman, J.D., S.W. Andrews, S. Painter and P. Stashenko, 1989. Adaptive changes in the strain Streptococcus mutans during colonization of the oral cavity. Microbiol. Ecol. Health Dis., 2: 231-239.
Direct Link - Hoshino, T., T. Izumi, T. Ooshima and T. Fujiwara, 2005. Method for rapid identification of oral streptocci by PCR using 16S-23S ribosomal RNA intergenic spacer gene. Pediatric Dental J., 15: 185-190.
Direct Link - Johnson, N.W., M. Glick and T.N.L. Mbuguye, 2006. Oral health and general health. Adv. Dental Res., 19: 118-121.
Direct Link - Kilian, M., L. Mikkelsen and J. Henrichsen, 1989. Taxonomic study of viridans streptococci: Description of Streptococcus gordonii sp. nov. and emended descriptions of Streptococcus sanguis (White and Niven 1946), Streptococcus oralis (Bridge and Sneath 1982) and Streptococcus mitis (Andrewes and Horder 1906). Int. J. Syst. Bacteriol., 39: 471-484.
Direct Link - Li, X.J., K.M. Kolltveit, L. Tronstad and I. Olsen, 2000. Systemic diseases caused oral infection. Clin. Microbiol. Rev., 13: 547-558.
Direct Link - Meurmann, J.H., M. Sanz and S.J. Janket, 2004. Oral health, atherosclerosis and cardiovascular disease. Crit. Rev. Oral Biol. Med., 15: 403-413.
Direct Link - Muto, M., Y. Hitomi, A. Ohtsu, H. Shimada, Y. Kashiwase, H. Sasaki, S.Yoshida and H. Esumi, 2000. Acetaldehyde production by non-pathogenic Neisseria in human oral microflora: Implications for carcinogenesis in upper digestive tract. Int. J.Cancer, 88: 342-350.
Direct Link - Pallares, R., A. Fenoll, J. Liñares, E. García and J. Casal et al., 2003. The epidemiology of antibiotic resistance in Streptococcus pneumoniae and the clinical relevance of resistance to cephalosporins, macrolides and quinolones. Int. J. Antimicrob. Agents, 22: S15-S24.
Direct Link - Ogunniyi, A.D., K.S. LeMessurier, R.M.A. Graham, J.M. Watt, D.E. Briles, U.H. Stroeher and J.C. Paton, 2007. Contributions of pneumolysin, pneumococcal surface protein A (PspA), and PspC to pathogenicity of Streptococcus pneumoniae D39 in a mouse model. Infec. Immun., 75: 1843-1851.
Direct Link - Renvert, S., 2003. Destructive periodontal disease in relation to diabetes mellitus, cardiovascular disease, osteoporosis and respiratory disease. Oral Health Prev. Dent., 1: 341-357.
Direct Link - Rudney, J.D. and C.J. Larson, 1993. Species identification of oral viridans Streptococii by Restriction Fragment Polymorphism of rRNA genes. J. Clin. Microbiol., 31: 2467-2473.
Direct Link - Socransky, S.S., C. Smith and A.D. Haffajee, 2002. Subgingival microbial profiles in refractory periodontal disease. J. Clin. Periodontol., 29: 260-268.
Direct Link - Tardiff, G., M.C. Sulavik, G.W. Jones and D.B. Clewell, 1989. Spontaneous switching of the sucrose-promoted colony phenotype in streptococcus sanguis. Infect. Immun., 57: 3945-3948.
Direct Link - Willcox, M.D.P., D.B. Drucker, V.F. Hillier and R.M. Green, 1985. Relationship of adhesion in vitro and cariogenicity of oral Streptococcus species in germ-free rats. Arch Oral Biol., 33: 635-636.
Direct Link - Wilson, W., K.A. Taubert, M. Gewitz, P.B. Lockhart and L.M. Baddour et al., 2007. Prevention of infective endocarditis. Circulation, 116: 1736-1754.
Direct Link - Xu, P., J.M. Alves, T. Kitten, A. Brown and Z. Chen et al., 2007. Genome of the opportunistic pathogen Streptococcus sanguis. J. Bacteriol., 189: 3166-3175.
Direct Link - Rossmann, S.N., P.H. Wilson, J. Hicks, B. Carter and S.G. Cron, 1998. Isolation of Lautropia mirabilis from oral cavities of human immunodeficiency virus-infected children. J. Clin. Microbiol., 36: 1756-1760.
PubMedDirect Link - Schentag, J.J., J.M. Hyatt, J.R. Carr, J.A. Paladino, M.C. Birmingham, G.S. Zimmer and T.J. Cumbo, 1998. Genesis of Methicillin-Resistant Staphylococcus aureus (MRSA), how treatment of MRSA infections has selected for vancomycin-resistant Enterococcus faecium and the importance of antibiotic management and infection control. Clin. Infect. Dis., 26: 1204-1214.
Direct Link