
A.A. Hemeida
Genetic Engineering and Biotechnology Research Institute (GEBRI), Sadat City Branch, Minufiya University, Minufiya, Egypt
M. Osman
Genetic Engineering and Biotechnology Research Institute (GEBRI), Sadat City Branch, Minufiya University, Minufiya, Egypt
M. El-Shahat
Genetic Engineering and Biotechnology Research Institute (GEBRI), Sadat City Branch, Minufiya University, Minufiya, Egypt
Medhat H. Hashem
Genetic Engineering and Biotechnology Research Institute (GEBRI), Sadat City Branch, Minufiya University, Minufiya, Egypt
Amal Mahmoud
Genetic Engineering and Biotechnology Research Institute (GEBRI), Sadat City Branch, Minufiya University, Minufiya, Egypt
Hosni Dahi
Genetic Engineering and Biotechnology Research Institute (GEBRI), Sadat City Branch, Minufiya University, Minufiya, Egypt
International Journal of Virology
Year: 2011 | Volume: 7 | Issue: 3 | Page No.: 91-99







ABSTRACT
Ninety-two positive samples for anti-HCV antibodies were selected from out patients of Center of Cardiac and Digestive System, Sohag, Egypt aged from 20 to 55 years. Then, confirmed by Reverse Transcription Polymerase Chain Reaction (RT-PCR) for HCV. The confirmed patients were received 12 vials of BEG IFN-2a for 12 weeks (180 IU mL-1 weekly) plus ribavirin (1000 mg for ≤75 kg or 1200 mg for >75 kg-Roche) and follow up by RT-PCR. The results showed that 67 patients (72.8%) responded to the treatment (group A) while 25 patients (27.2%) non responders (group B). The two groups were Screened for Serum Alanine Transaminase (ALT), Serum Aspartate Transaminase (AST), Serum Alpha Fetoprotein (AFP), serum albumin, serum creatinine, Serum TSH, Hemoglobin (Hb), White Blood Cells Count (WBCs) and Platelets count. Hematological disorders and ALT elevation were common side effects of treatment. The side effects were increased within group B than that of group A. Three random Hepatitis C Virus (HCV) samples from group B were studied for the diversity and sequence variations. Sequencing of 223 nucleotide of 5'-untranslated region (5'-UTR) was performed. In the phylogenetic analysis, the three sequences and 80 sequences of HCV different genotypes from GenBank were used. Nucleotide variations were found in 7 (3.14%) of the 223 nucleotide positions analyzed. The variations were observed in the nucleotides (74, 92, 112, 113, 133, 172 and 180). Nucleotide insertion was seen in one sequence in the nucleotide position of 212. Root Neighbor-joining (NJ) tree revealed that the three HCV samples could be classified as genotype 4. Two of the three samples were closely related (98.2%) while the third clustered with isolate from Gabon (98.7%). The third isolate may be a new subtype but this will require an in-depth exploration on sequence variability in at least two coding regions.
PDF Abstract XML References Citation
Received: June 19, 2011;
Accepted: July 23, 2011;
Published: October 20, 2011
How to cite this article
A.A. Hemeida, M. Osman, M. El-Shahat, Medhat H. Hashem, Amal Mahmoud and Hosni Dahi, 2011. Genetic Variations in a Conserved 5'-untranslated Region of Hepatitis C Virus Isolated from Egypt. International Journal of Virology, 7: 91-99.
DOI: 10.3923/ijv.2011.91.99
URL: https://scialert.net/abstract/?doi=ijv.2011.91.99
DOI: 10.3923/ijv.2011.91.99
URL: https://scialert.net/abstract/?doi=ijv.2011.91.99
INTRODUCTION
Hepatitis C Virus (HCV) is a major health problem affecting 170 million people worldwide. The seroprevalence rate is about 1% in western countries and North America, 3-4% in some Mediterranean and Asian countries and up to 10-20% in parts of central Africa and Egypt (WHO, 2000; Abdel-Hamid et al., 2007).
Egypt has the highest prevalence of HCV worldwide, where it infects about 15% of the general population (Egyptian Ministry of Health, 2007).
The infection with the HCV is the leading cause of chronic hepatitis worldwide, progressing to liver cirrhosis in approximately 20% of patients after 10 years and to Hepatocellular Carcinoma (HCC) in a subset of them with a yearly incidence of 3% (Zein, 2000).
HCV is an RNA virus and a member of the Hepacivirus genus classified into the Flaviviridae family. HCV presents high mutation rates and because of that it has been evolved to different genotypes based on nucleotide sequence heterogeneity and classified in six major genotypes and more than 80 subtypes (Mizokami et al., 1996; De Lamballerie et al., 1997; Robertson et al., 1998; Simmonds et al., 2005). The importance of determining the HCV genotype has increased since several investigators have described a significant correlation between hepatitis C virus genotype and response to interferon treatment or disease severity (Dammacco et al., 2000; Farci and Purcell, 2000; Yasmeen et al., 2009).
The current standard of care in previously untreated patients with chronic hepatitis C is combination therapy with pegylated interferon alpha and ribavirin (Patel and McHutchison, 2004). Standard IFN-a monotherapy results in only 10% sustained virological response while pegylated IFN-a plus ribavirin combination therapy improves the sustained virological response to 54-56% (Walker et al., 2003). The combination of pegylated interferon alfa plus ribavirin is currently the standard therapy for chronic hepatitis C infection in adults. Substained virologic response is achieved in 44-75% of patients depending on genotype (Hasan et al., 2004).
Leucopenia and other hematological disorders are common side effects of pegylated interferon alfa plus ribavirin treatment (Manns et al., 2001).
The variability of HCV-RNA is more prominent in E1 and E2 regions; sequence of core gene and non-structural regions like NS3 often remains conserved. The lowest sequence variability between genotypes is found in the 5'-untranslated region (5`-UTR) (Simmonds et al., 2005). The 5'-UTR of HCV is an essential component of the Internal Ribosome Entry Site (IRES) that regulates Cap-independent translation of HCV (Wang et al., 1994).
The present study aimed at an in-depth analysis of sequence variability in a well conserved region of 5`-UTR of HCV from Sohag governorate-Egypt. The selected samples were analyzed by phylogenetic analysis to confirm the extent of variations in the 5`-UTR of HCV isolates.
MATERIALS AND METHODS
Patients: Ninety-two positive samples for anti-HCV antibodies were selected from out patients of Center of Cardiac and Digestive System, Sohag, Egypt aged from 20 to 55 years.
Reverse transcription-PCR (RT-PCR)
HCV RNA extraction: RNA was extracted from all samples (140 μL) by using of the QIAamp viral RNA Extraction Kit (Qiagen, Cat. No 52904) according to manufacturer’s instructions. In brief, samples were lysed and the RNA was captured on the spin columns provided. The RNA was washed, eluted and then stored at -20°C until used in PCR amplification.
RT-PCR: The 5`-UTR of HCV was amplified by using One Step RT-PCR Kit (Qiagen, cat. No. 210210). The QIAGEN One Step RT-PCR Kit is designed to be used with gene-specific primers (Cat. No. P-6A100 and P-6B100). The master mix typically contains all the components required for RT-PCR except the template RNA. The reactions were performed in 25 l total volume consist of the master mix plus template RNA according to kit instructions.
The 5`-UTR of HCV RNA amplification was performed by using of the Gene Amp PCR system 2400 (Biometra) programmed for 35 cycles. PCR products were visualized on 1% agarose using UV-trans-illuminator and photographed by a digital camera (FUJI 100) with orange filter.
Biochemical and Hematological study: The RT-PCR confirmed patients for HCV received 12 vials of pegylated IFN alpha-2a for 12 weeks (180 mcg 0.5 mL-1; fixed dose/week-Roche) plus ribavirin (1000 mg for ≥75 kg or 1200 mg for >75 kg-Roche) and followed up by RT-PCR.
Sixty-seven patients responded to the treatment (group A) while twenty-five patients did not respond (group B). All patients of group A and B were Screened for Serum Alanine Transaminase (ALT), Serum Aspartate Transaminase (AST), Serum Alpha Fetoprotein (AFP), Serum Albumin, Serum Creatinine, Serum TSH, Blood Hemoglobin (Hb), White Blood Cells Count (WBCs) and Platelets count.
Sequence analysis: Three random HCV samples from group B were studied for the diversity and sequence variations. DNA sequencing was carried out with the BigDye® Terminator v3.1 Cycle Sequencing Kit and an Applied Biosystems 373xl DNA Analyzer. DNA sequencing was carried out using the PCR product specific primers. The sequence analysis was performed using the Finch TV 1.4 Software.
Sequences were compared to the sequences of GenBank database using BLAST software (NCBI). Clustal W 1.81 and MEGA 4 software were used for multiple alignment and phylogeny construction. Phylogenetic analysis of 5-UTR sequences was carried out to analyze the distribution of different HCV isolates. At least 80 sequences of HCV different genotypes from GenBank were used to construct Neighbor-joining (NJ) tree by using MEGA software. Bootstrapping of 1000 replicas was carried out (Felsenstein, 1985).
Statistical analysis: Biochemical and Hematological data were analyzed by Excel and SPPS package programs
RESULTS
Clinical characteristics
Group A: From the RT-PCR confirmed patients for HCV (Fig. 1), Sixty-seven patients (72.8%) responded to the treatment of IFN plus ribavirin, in which 53 males and 14 females. As shown in Table 1, leucopenia affected 40.29% (≤3000 cells/mm3), Hemoglobin decreased in 35.82% (≤11.9 g dL-1 for male but ≤10.9 g dL-1 for female), Thrombocytopenia was observed in 34.32% (≤130000 cells/mm3) and ALT elevation in 14.92% of these patients.
Group B: Twenty-five patients (27.2%) did not respond to the treatment, (20 males and 5 females). As shown in Table 1 some side effects occurred including leucopenia (72%, ≤3000 cells/mm3), Hemoglobin decreased (72%, ≤11.9 g dL-1 for male but ≤10.9 g dL-1 for female), Thrombocytopenia (72%, ≤130000 cells/mm3) and ALT elevation (40%).
Factors of group A and B: After the 12th week of treatment, 67 patients responded to the treatment (Group A) whereas 25 patients non responders (Group B) in this period. Hematological disorders and ALT elevation were common side effects of treatment. The side effects increased within group B than that of group A as illustrated in Table 1.
 | |
| Fig. 1: | Ethidium bromide stained agarose gel electrophoresis of HCV 5'-UTR amplification by RT-PCR, M:100 bp DNA ladder, lane 1: negative control, lane 2 : positive control and Lanes 3 to 7: PCR-positive results (bands sizing 270 bp in each) |
| Table 1: | Parameters of group A (responders) and group B (non responders) to IFN alpha-2a plus ribavirin treatment |
 | |
| Table 2: | Factors playing a role in the effectiveness of interferon therapy in patients with chronic hepatitis C according to their response to IFN-α therapy |
 | |
| · Insignificant at p>0.05, * Significant at p<0.05 | |
Statistically, the two groups of patients were similar with respect to clinical characteristics except Creatinine (p = 0.044*) and age (p = 0.03*) as shown in Table 2.
2. 5'-UTR sequence analysis: Three random serum samples from HCV group B patients were studied for the diversity and sequence variations. These sera samples from patients living in Akhmeem, Monshaa and Maragha.
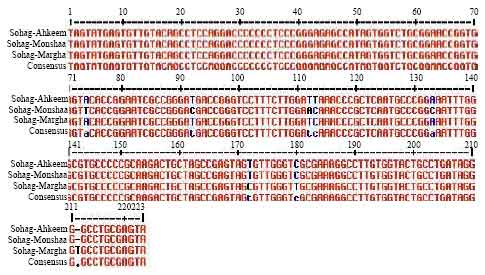 | |
| Fig. 2: | Nucleotide sequence comparison of HCV 5'-UTR region between Sohag isolates (Sohag-Akhmeem, Sohag-Monshaa and Sohag-Maragha) |
| Table 3: | The similarity and divergence between Sohag HCV isolates and different genotypes of HCV |
 | |
| -Percent Similarity in upper triangle. -Percent Divergence in lower triangle | |
Sequencing of 223 nucleotides of 5'-UTR from PCR product was performed. Seven nucleotide variations were found between sohag samples at positions 74, 92, 112, 113, 133, 172 and 180. One nucleotide insertion was detected in Sohag-Maragha at position 212 (Fig. 2). In multi-alignment analysis, the three sequences and 80 sequences of HCV different genotypes from GenBank were used. Different variations at different positions in 5'-UTR of HCV were observed.
According to the phylogenetic tree (Fig. 3), the three isolates (Sohag-Akhmeem, Sohag-Monshaa and Sohag-Maragha) were classified as genotype 4. When Sohag-Monshaa was compared with Sohag-Maragha and Sohag-Akhmeem, the similarity was 96.9 and 97.8% respectively Table 3. Sohag-Akhmeem and Sohag-Maragha were closely related (98.2%) (Cluster 1) while Sohag-Monshaa clustered with L29619.1 isolate from Gabon and reported by Lieven et al. (1994), the similarity was 98.7% (Cluster 2).
Multi-alignment of 5'UTR sequences of Sohag non-responders samples with other Egyptian patients who responded (Zekri et al., 2007) deposited in GenBank were done.
 | |
| Fig. 3: | Neighbor-joining (NJ) tree of GenBank and sohag samples. Bootstrapping of 1000 replicates |
One nucleotide variation was found at position 153, nucleotide deletion was detected in sohage isolates at position nine and two nucleotides insertion was detected at positions 30 and 117.
DISCUSSION
In this study, HCV infection of ninety-two patients who were positive for anti-HCV antibodies, was confirmed by RT-PCR for HCV. These patients received 12 vials of pegylated IFN alpha-2a plus ribavirin for 12 weeks and were followed up by RT-PCR.
The results showed that 67 patients (72.8%) responded to the treatment while 25 patients (27.2%) non-responders. The combination of pegylated interferon alfa plus ribavirin is currently the standard therapy for chronic hepatitis C infection in adults. Substained virologic response is achieved in 44-75% of patients depending on HCV genotype (Hasan et al., 2004). Sixty-seven patients responder to the treatment. On the other hand, twenty-five patients were non-responders. Leucopenia and other hematological disorders are common side effects of this antiviral treatment (Manns et al., 2001). These side effects may prevent physicians from continuing their patients on interferon therapy or reducing dosage (Turbide et al., 2008).
The two groups of patients showed no significant difference with respect to clinical laboratory findings characteristics except S. creatinine (p = 0.044*) and age (p = 0.03*). Ribavirin is mainly cleared by the kidneys and plasma concentrations are determined by renal function (Bruchfeld et al., 2002). Mild renal effects have been reported during the first few days of interferon alfa therapy and may cause fever. Nephritic syndrome and severe injury are rare (Dusheiko, 1997).
On the other hand, the importance of determining the HCV genotype has increased since several investigators have described a significant correlation between hepatitis C virus genotype and response to interferon treatment or disease severity (Dammacco et al., 2000; Farci and Purcell, 2000; Yasmeen et al., 2009).
In the present study, three random HCV samples from non-responders patients were studied for the diversity and sequence variations in the conserved 5'-UTR. The 5'-UTR was selected because of its importance as an essential component of the Internal Ribosome Entry Site (IRES) that regulates Cap-independent translation of HCV (Wang et al., 1994).
Sequence of 223nt of HCV 5'-UTR of Sohag samples was used. Seven nucleotide variations were found between the three samples and one nucleotide insertion was detected in one sample (Sohag-Maragha). Also, different variations at different positions in 5'-UTR of HCV were observed between the three sequences of sohag samples and the sequences of HCV different genotypes and Egyptian responders ones from GenBank. Nucleotide substitution within the HCV 5`-UTR may influence the viral translation and its sensitivity to the antiviral action of interferon (Yasmeen et al., 2009).
Sequence alignment between Sohag and GenBank isolates was done, different variations at different positions between samples were observed. HCV variants were classified at six genotypes and more than 80 subtypes. The lowest sequence variability between different genotypes was found in the 5`UTR, where specific sequences and RNA secondary structure are required for replication and translation function (Simmonds et al., 2005).
Rooted Neighbor-joining (NJ) tree revealed that the three HCV samples classified as genotype 4. Two of the three samples were closely related (Sohag-Akhmeem and Sohag-Maragha) and the similarity was 98.2%. While the third (Sohag-Monshaa) clustered with sample from Gabon (98.7%). Simmonds et al. (2005) reported that subtypes 4a (55%), 4 (24%), 4o (7%), 4m (3%),4l (3%) and 4n (2%) were distributed in Gabon whereas subtypes 4c (36%), 4h (15%), 4e (13%), 4(13%),4g(13%), 4f(5%), 4a(2.6%) were distributed in Egypt. The third sample of sohag may be a new subtype. Such observations need to be confirmed and substantiated by further investigations using more than one approach.
Lieven et al. (1994) observed a specific recognition sequence in the 5'UTR region for every newly identified subtype. A new subtype will require an in-depth exploration on sequence variability in at least two coding regions (Simmonds et al., 1994).
However, this study describes the presence of unique sequence variability in the 5'-UTR of hepatitis C virus genotype 4, isolated from treatment non-responders patients from Egypt Mutations found in these unique sequences may lead to find a method for response and non-response prediction of HCV patients.
REFERENCES
- Abdel-Hamid, M., M. El-Daly, V. Molnegren, S. El-Kafrawy and Abdel-Latif et al., 2007. Genetic diversity in hepatitis C virus in Egypt and possible association with hepatocellular carcinoma. J. Gen. Virol., 88: 1526-1531.
CrossRefDirect Link - Yasmeen, A., A.A. Siddiqui, S. Hamid, T. Sultana, W. Jafri and M.A. Persson, 2009. Genetic variations in a well conserved 5-untranslated region of hepatitis C virus genome isolated in Pakistan. J. Virol. Methods., 160: 38-47.
PubMed - Bruchfeld, A., K. Lindahl, R. Schvarcz and L. Stahle, 2002. Dosage of ribavirin in patients with hepatitis C should be based on renal function: A population pharmakokinetic analysis. Ther. Drug Monit., 24: 701-708.
PubMed - Dammacco, F., D. Sansonno, C. Piccoli, V. Racanelli, F.P. D'Amore and G. Lauletta, 2000. The lymphoid system in HCV infection: Autoimmunity, mixed cryoglobulinemia and over B-cell malignancy. Semin. Liver Dis., 20: 143-157.
PubMed - De Lamballerie, X., R.N. Charrel, H. Attoui and P. De Micco, 1997. Classification of hepatitis C virus variants in six major types based on analysis of the envelope 1 and nonstructural J. Gen. Virol., 78: 45-51.
PubMed - Dusheiko, G., 1997. Side effects of alpha interferon in chronic hepatitis C. Hepatology, 26: 112S-121S.
PubMed - Farci, P. and R.H. Purcell, 2000. Clinical significance of hepatitis C virus genotypes and quasispecies. Semin. Liver Dis., 20: 103-126.
PubMed - Felsenstein, J., 1985. Confidence limits on phylogenies: An approach using the bootstrap. Evolution, 39: 783-791.
CrossRefDirect Link - Stuyver, L., W. van Arnhem, A. Wyseur, F. Hernandez, E. Delaporte and G. Maertens, 1994. Classification of hepatitis C viruses based on phylogenetic analysis of the envelope 1 and nonstructural 5B regions and identification of five additional subtypes. Proc. Natl. Acad. Sci. USA., 91: 10134-10138.
Direct Link - Manns, M.P., J.G. McHutchison, S.C. Gordon, V.K. Rustgi and M. Shiffman et al., 2001. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: A randomised trial. Lancet, 358: 958-965.
CrossRefPubMedDirect Link - Mizokami, M., T. Gojobori, K. Ohba, K. Ikeo and X.M. Ge et al., 1996. Hepatitis C virus types 7, 8 and 9 should be classified as type 6 subtypes. J. Hepatol., 24: 622-624.
Direct Link - Patel, K. and J.G. McHutchison, 2004. Initial treatment for chronic hepatitis C: Current therapies and their optimal dosing and duration. Cleve. Clin. J. Med., 71: S8-12.
PubMed - Robertson, B., G. Myers, C. Howard, T. Brettin and J. Bukh et al., 1998. Classification, nomenclature and database development for hepatitis C virus (HCV) and related viruses: Proposals for standardization. Arch. Virol., 143: 2493-2503.
PubMed - Simmonds, P., D.B. Smith, F. McOmish, P.L. Yap and Kolberg et al., 1994. Identification of genotypes of hepatitis C virus by sequence comparisons in the core, E1 and NS-5 regions. J. Gen. Virol., 75: 1053-1061.
PubMed - Simmonds, P., J. Bukh, C. Combet, G. Deleage and N. Enomoto et al., 2005. Consensus proposals for a unified system of nomenclature of hepatitis C virus genotypes. Hepatology, 42: 962-973.
PubMed - Turbide, C., C. Soulellis, M. Deschenes and N. Hilzenrat, 2008. Does a decline in the hematological and biological parameters induced by interferon and ribavirin combination therapy for the hepatitis C virus predict a sustained viral response?. Can. J. Gastroenterol., 22: 149-152.
PubMed - Walker, M., T. Appleb, W. Zhong, J. Lau and Z. Hong, 2003. Review hepatitis C virus therapies: current treatments, targets and future perspectives. Antivir. Chem. Chemother., 14: 1-21.
Direct Link - Wang, C.Y., P. Sarnow and A. Siddiqui, 1994. A conserved helical element is essential for internal initiation of translation of hepatitis C virus RNA. J. Virol., 68: 7301-7307.
Direct Link - Zein, N., 2000. Clinical significance of hepatitis C virus genotypes. Clin. Microbiol. Rev., 13: 223-235.
PubMed