
Ajay Behra
Rungta College of Pharmaceutical Sciences and Research, Kohka-Kurud Road Bhilai, Chhattisgarh, India
Tapan Kumar Giri
Rungta College of Pharmaceutical Sciences and Research, Kohka-Kurud Road Bhilai, Chhattisgarh, India
Dulal Krishna Tripathi
Rungta College of Pharmaceutical Sciences and Research, Kohka-Kurud Road Bhilai, Chhattisgarh, India
Ajazuddin
Rungta College of Pharmaceutical Sciences and Research, Kohka-Kurud Road Bhilai, Chhattisgarh, India
Amit Alexander
Rungta College of Pharmaceutical Sciences and Research, Kohka-Kurud Road Bhilai, Chhattisgarh, India
International Journal of Pharmacology
Year: 2012 | Volume: 8 | Issue: 5 | Page No.: 283-305







ABSTRACT
As compared to both injectable and oral delivery, the buccal delivery is preferred to and advantageous for enhancement of bioavailability of drug. The mucosal surfaces are usually rich in blood supply and provide the means for rapid drug transport to the systemic circulation avoiding drug degradation in harsh gastric environment and first-pass hepatic metabolism. Besides, it can prolong absorption and residence time due to prolonged contact with absorption surface and with the site of application allowing once or twice daily dosing. A rapid onset of action with comfort and convenience in delivery of certain drugs has been observed. Many drugs have been tried with buccal route, a few are also available commercially. Clinical need should be significant and must be high enough to counterbalance the high cost associated with development of a buccal product. Buccal drug delivery assures four times the absorption rate from the skin. The review aims the development in the buccal adhesive drug delivery systems to provide basic principles to the young researchers which will be helpful in overcoming the difficulties associated with the formulation design.
PDF Abstract XML References Citation
Received: January 24, 2012;
Accepted: March 05, 2012;
Published: June 13, 2012
How to cite this article
Ajay Behra, Tapan Kumar Giri, Dulal Krishna Tripathi, Ajazuddin and Amit Alexander, 2012. An Exhaustive Review on Recent Advancement in Pharmaceutical Bioadhesive Used for Systemic Drug Delivery Through Oral Mucosa for Achieving Maximum Pharmacological Response and Effect. International Journal of Pharmacology, 8: 283-305.
DOI: 10.3923/ijp.2012.283.305
URL: https://scialert.net/abstract/?doi=ijp.2012.283.305
DOI: 10.3923/ijp.2012.283.305
URL: https://scialert.net/abstract/?doi=ijp.2012.283.305
INTRODUCTION
There are various route of drug administration and each route has its own limitations. (Hoogstraate and Wertz, 1998). Oral route for delivery of drug, although more convenient, causes major problems like hepatic first pass metabolism (Patel et al., 2011a; Abdollahi et al., 2003) degradation of drug in harsh gastrointestinal environment (Kulkarni and Desai, 2010) and poor bioavailability (Dharani and Shayeda, 2010; Jafar and Ali, 2011). This route shows inadequate and erratic absorption (Sudhakar et al., 2006). Parenteral route for drug administration avoids this problem but it has also some drawback like pain at the site of administration, anaphylaxis and extravasation infection (Scholz et al., 2008; Qureshi et al., 2006), so oral cavity is selected for administration of macromolecules such as oligopeptides (Veuillez et al., 2001), unstable proteins and polysaccharides (Gandhi et al., 2011). Administration through oral cavity can be used as an attractive and alternative site for drug delivery which can facilitate particularly in overcoming deficiencies associated with frequent dosing (Wong et al., 1999).
The oral mucosa is comparatively permeable and enriched with blood supply (Shojaei, 1998), it is highly vascularized (Rossi et al., 2005), vigorous and demonstrate short recovery time after stress or damage (Yamamoto et al., 2001). For drug absorption the total surface area of membrane of oral cavity available is 100-170 cm2 (Tayal and Jain, 2011; Miller et al., 2005) of which 50 cm2 represent buccal cavity consisting of liner mucosa (Lee et al., 2000). The thickness of buccal epithelium is approximately 500-800 μm (Harris and Robinson, 1992).
Local therapy is used to treat condition such as gingivitis, oral candidiasis (infection by fungus Candida albicans), oral lesions (breaking of mucous membrane due to disease), dental carries (decaying of teeth), xerostomia (dryness of mouth due to lack of saliva), oral cancer, mucositis and neuropathic pain (Galati et al., 2000; Smart, 2004; Pourhashemi et al., 2007; Taliyan and Sharma, 2010).
For transmucosal drug delivery buccal and sublingual or floor of mouth (Hoogstraate et al., 1996; Kowsalya et al., 2011), areas are most commonly used route. Sublingual mucosa is more permeable, thinner with high blood flow than buccal mucosa. Due to its smooth and relatively immobile surface, the buccal mucosa offer sustained and controlled delivery of drug (Madhav et al., 2009) and less permeability (Shakya et al., 2011).
Flexible, elastic and soft patches are used for buccal delivery (Patel et al., 2001; Patel and Poddar, 2009) for modified release dosage form (Parmar et al., 2010). Compared to tablet buccal patches are of small size and with adequate thickness to provide better patient compliance (Morales and McConville, 2011).
ADVANTAGES OF BUCCAL DRUG DELIVERY
| • | As it by passes the GIT and hepatic portal system, it protects the drug from degradation due to pH and various enzyme present in GIT. The bioavailability of orally administrated drug is increased (Vinod et al., 2010) |
| • | Patient compliance is improved due to the elimination of associated pain with injections. Drugs can be administered to mentally ill, disabled and uncooperative, or unconscious or incapacitated patients conveniently (Miller et al., 2005) |
| • | Allows localization of the drug for a prolonged period of time as required for sustained and controlled drug delivery (Grabowski et al., 1992; Trivedi et al., 2011) |
| • | Dose dependent side effect are reduced due to dose reduction |
| • | Unlike other surfaces for transdermal drug delivery, mucosal surfaces exhibit a faster initiation and decline of delivery than other transdermal patches as it does not have stratum corneum, a major barrier layer for drug transport (Gupta et al., 2011; Varshosaz et al., 2006) |
| • | Flexibility in physical state, shape, size and surface |
| • | Low metabolic activity (Gangwar, 2011) |
| • | Very rare incidents of nausea and vomiting have been reported (Mohammadi and Seyedi, 2008) |
| • | Drugs with poor bioavailability and the drugs which are unstable at different pH can be administrated conveniently by this route (Amarji et al., 2007; Giri et al., 2010a) |
| • | Though, less permeable than the sublingual area, drugs can be rapidly absorbed into the venous system below the oral mucosa because it is well vascularized,. Unlike rectal and transdermal route the drug dissolution is relatively large due to the presence of saliva (Patel et al., 2011b) |
LIMITATION OF BUCCAL DELIVERY
| • | Drugs which are unstable at buccal pH (5.5-7) cannot be administered (Vyas and Khar, 2008) |
| • | Restriction in eating and drinking may be required (Lalla and Gurnancy, 2002) |
| • | Due to over hydration, the structural integrity of the formulation may get disrupted leading to slippery surface and hydration of bioadhesive polymer (Jain, 2002; Shanker et al., 2009) |
| • | The area of absorptive membrane is relatively lesser. If the effective area for absorption is dictated by the dimensions of a delivery system, this area then becomes even smaller (Alur et al., 2002) |
| • | Drugs with large dose are difficult to be administered (Khairnar and Sayyad, 2010) |
| • | Only those drugs which are absorbed by passive diffusion can be administered by this route |
| • | Frequent dosing may be required for drugs intended for local action but may face rapid elimination due to the flushing action of saliva or the ingestion of foods stuffs (Yousefzadeh et al., 2006; Wani et al., 2007) |
| • | Low permeability of the buccal membrane, specifically when compared to the sublingual membrane (Peppas and Buri, 1985) |
OVERVIEW OF ORAL MUCOSA
Anatomy of oral mucosa: The oral cavity comprises the lip, cheek, tongue, hard palate, soft palate and floor of mouth as shown in Fig. 1. The oral mucosa divided in three distinctive layer which are outer epithelium, middle basement and inner connective tissues as shown in Fig. 2.
There are two parts of oral cavity; the space between teeth and cheeks or lips is outer oral vestibule while the space between teeth and pharynx is interior oral vestibule (Tortora, 2002). The outer layer of buccal mucosa is composed of approximately 40-50 layers of stratified squamous epithelial cell while the sublingual epithelium contains fewer layers (Gandhi and Robinson, 1988). This layer serves as protective covering for the tissue and acts as a barrier to the entry of foreign material (Ghosh and Pfister, 2005), like antigens, carcinogens, microbial toxin and enzyme from food and beverages. The middle layer, a basement membrane, is a continuous layer of extracellular material and forms a boundary between the basal layer of epithelium and connective tissue (Senthil et al., 2007; Shojaei, 1998; Basu et al., 2010). The epithelium in masticatory mucosa are keratinized and lining mucosa are non-keratinized. The lining mucosa contributes approximately 60%, the masticatory mucosa contributes 25% and the specialized mucosa occupies approximately 15% of the total surface area of oral mucosa lining in an adult human. As compared to masticatory mucosa, the lamina propria of lining mucosa is lesser in thickness and elasticity.
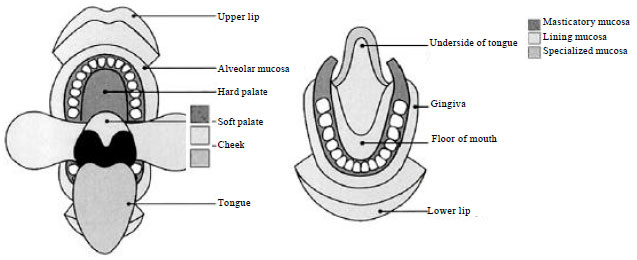 | |
| Fig. 1: | Schematic representation of the different linings of mucosa in mouth (Patel et al., 2011a) |
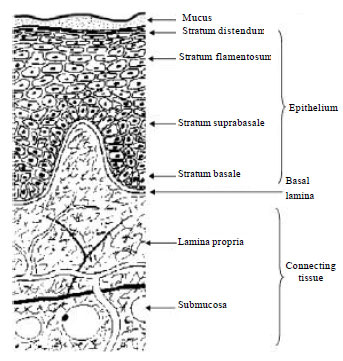 | |
| Fig. 2: | Cross-section of buccal mucosa (Sudhakar et al., 2006) |
The specialized mucosa possesses well papilated surface both keratinized and non-keratinized (Collins and Dawes, 1987; Ahmed et al., 2011).
Biochemistry of oral mucosa: The keratinized cell of epidermis of skin and masticatory mucosa of oral cavity is a barrier for drug permeability. In general, keratinized and non-keratinized epithelium of oral cavity occupies about 50% and 30%, respectively (Collins and Dawes, 1987). The composition and state of keratinization of oral mucosa is shown in Table 1.
Secretion of oral cavity
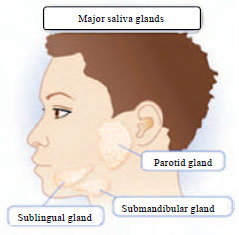
Saliva: The physiological environment of the oral cavity in terms of pH, fluid volume and composition, depends on the secretion of saliva (Herrera et al., 1988; Pajoumand et al., 2003). There is a salivary coating over mucosal surface having thickness of about 70 μm. This acts like a stagnant layer. Three major salivary glands- parotid, submandibular and sublingual and minor salivary or buccal glands situated in or immediately beneath the mucosa secrete the saliva (Slomiany et al., 1996; Abdollahi et al., 2003). The paired parotid glands, the major salivary glands, are located opposite to the maxillary first molars and the submandibular and sublingual glands as shown in Fig. 3 are located in the floor of the mouth. Minor salivary or buccal glands are found in the lower lip, tongue, palate, cheeks and pharynx (Humphrey and Russell, 2001). Watery secretion is produced by the parotid and submaxillary glands while the main viscous saliva with limited enzymatic activity is secreted by sublingual glands(Slomiany et al., 1996; Herrera et al., 1988). Except for the gums and the anterior part of the hard palate these glands are placed at every region of the mouth (Llena-Puy, 2006; Giradkar et al., 2010).
There are several compounds in the saliva that control the mouth hemiparasites. The major constituent, about 99% is water with 1% organic and inorganic materials. The composition of the saliva depends mostly on the flow rate along with three other factors: the time of day, the type of stimulus and the degree of stimulation. Its pH varies from 5.5-7 depending on the flow rate. The concentrations of sodium and bicarbonate increase when flow of saliva increases resulting to an increase in the pH. Saliva imparts major effect on many activities like mastication, speech and tissue lubrication (Tabak et al., 1982; Malekipour et al., 2008; Rohaya et al., 2010).
| Table 1: | The composition and state of keratinisation of oral mucosa |
 | |
 | |
| Fig. 3: | Major salivary gland (Patricia et al., 2008) |
Saliva contains a high molecular weight mucin called MG1 that attaches to the surface of the oral mucosa and maintains hydration, provides lubrication and concentrates protective molecules such as secretory immunoglobulins and also limits the attachment of microorganisms.
Salivary glands consists of acinar and ductal cells. Acinar cells, present in parotid gland, are responsible for production of serous secretion. Most of the α-amylase is synthesized in this gland. The submandibular and sublingual glands produce mainly mucin while proline and histin are produced by parotid and submandibular glands. Mucous are essentially produced by the minor salivary glands (Nauntofte and Lagerlof, 2003; Saad et al., 2005; Chatterjee, 1985).
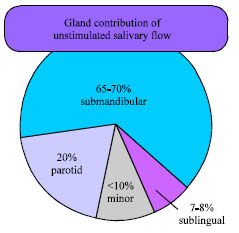
Clinical diseases and progonostic monitoring on human saliva has a great potential (Jessie et al., 2008). Saliva is complex mixture of fluids containing oral bacteria and food debris. The fluids along with gingival crevicular fluid come from the major and minor salivary glands. The average daily flow of whole saliva varies from 1-1.5 L depending on the health. The contributions of the salivary glands for usual flow are: 20% from parotid, 65% from submandibular, 7-8 % via sublingual and less than 10 % via humerous minor gland, shown in (Fig. 4) and when stimulated flow rate can increase by more than 50% of total salivary secretion (Edgar, 1990).
 | |
| Fig. 4: | Percentage contributions of the different salivary glands during unstimulated (Patricia et al., 2008) |
Mucus: The intercellular ground substance called mucus surrounds the epithelial cells of buccal mucosa varies in thickness ranging from 40-300 μm (Allen et al., 1984). Mucus, a translucent and viscid secretion, forms a thin, continuous gel cover over the mucosal epithelial surface like a blanket. It is secreted by the goblet cells lining the epithelia or by special exocrine glands with mucus cells acini. Mucus consists of about 95% water and the major organic component in mucus is glycoproteins (Ehrhardt and Kim, 1995; Zakaria et al., 2004).
The thickness of the mucus depends on its location (Marriot and Hughes, 1990). The thickness of the mucus blanket is controlled by the balance between the rate of secretion and the rate of degradation and shedding. Mucus secretion is greatly stimulated by toxic and irritating substances, the thickness of the mucus blanket is increased while the irritants go away from the epithelium efficiently and rapidly moving (Thomas and Moridani, 2009; Puchelle, 1987). The major and minor salivary glands secret mucus as part of saliva (Sangeetha et al., 2010). Up to 70% of the total mucin found in saliva is secreted by the minor salivary glands (Rathbone et al., 1994). The mucus network carries a negative charge at physiological pH due to the presence of sialic acid and sulfate residues which also play a role in mucoadhesion. At this pH mucus a strongly cohesive gel structure can be formed that will combine with the epithelial cell surface as a gelatinous layer.
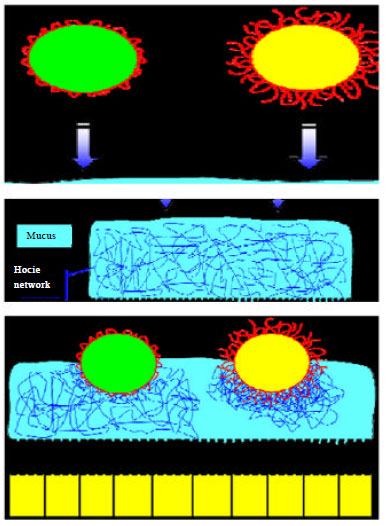 | |
| Fig. 5: | Mucus interaction with drug delivery system (Madhav et al., 2009) |
The interaction of mucus with drug delivery system is shown as Fig. 5 (Gandhi and Robinson, 1988).
ORAL MUCOSA A BARRIER TO PERMEABILITY
The rate and extent of drug absorption through the buccal mucosa can be retarded by the saliva, mucus, membrane coating granules, basement membrane, etc., which also act as barriers (Gandhi and Robinson, 1988). The oral mucosa in general is a somewhat spongy epithelia intermediate between that of the epidermis and intestinal mucosa. It has been observed that the permeability of the buccal mucosa is 4-4000 times greater than that of the skin (Galey et al., 1976). However, this value is not absolute, there are considerable differences in permeability between different regions of the oral cavity due to difference in structures and functions of the different oral mucosa (Harris and Robinson, 1992; Akhionbare and Ojehanon, 2007). In general, the permeability of the oral mucosa decreases in the order: sublingual<buccal<palatal (Harris and Robinson, 1992). The permeability coefficient has a direct relation with the membrane thickness (i.e., inverse to its thickness) degree of keratinisation of these tissues and with the physicochemical properties of the drug like molecular weight, size and lipophilicity. The characteristic features of oral mucosa are shown in Table 2 (Squlcr and Johnson, 1975).
Sublingual mucosa is relatively thin and non-keratinized, the buccal mucosa is thicker and non keratinized and the palatal mucosa is intermediate in thickness and is keratinized (Wertz and Squier, 1991). The permeability barrier property of the oral mucosa is mainly due to intercellular materials derived from the so called membrane coating granules (Gandhi and Robinson, 1994). Membrane coating granules are spherical or oval organelles with size range from 100-300 nm and are found in both keratinized and non-keratinized epithelia (Hayward, 1979).
| Table 2: | Characteristics features of oral mucosa |
 | |
| NK: Non-keratinized, K: Keratinized | |
The membrane coating lipids granules of keratinized epithelia include sphingomyelin, glucosyl ceramide, ceramide and other non-polar lipid. However, for non-keratinized epithelia the major membrane coating granules are lipid components e.g., cholesterol ester, cholesterol and glycosphingolipids (Ganem-Quintanar et al., 1997a). The membrane coating granules present on the basement membrane exhibit some resistance to permeation, however the outer epithelium is considered as rate limiting to mucosal penetration. The relatively large molecules cannot get excluded because of less dense structure of the basement membrane. (Slomiany et al., 1996).
DRUG DELIVERY VIA THE ORAL MUCOSA
The function and detailed description of the oral mucosa is available elsewhere but only those details which are relevant to the oral mucosal delivery of drug have been included here. Lips, cheek (buccal), tongue, hard palate, soft palate and floor of mouth are the parts of oral cavity (Dawes, 2007; Al-Bassiouny, 2009). Buccal and sublingual areas are the most appropriate site for drug delivery and these may be used for the treatment of local (Chiappin et al., 2007) disease like toothaches (Ishida et al., 1982), periodontal disease (Collins et al., 1989; Elkayam et al., 1988), bacterial and fungal infections (Samaranayake and Ferguson, 1994), aphthous (Nagai and Machida, 1985) and dental stomatitis (Nagai, 1985) or systemic diseases. The surface area of oral mucosa, skin and gastrointestinal tract are about 200, 20000 and 350000 cm2, respectively. However, the oral mucosa is highly vascularized and therefore any drug diffusing into the oral mucosal membranes has direct access to the systemic circulation via capillaries and venous drainage (Squier and Wertz, 1993; Hakan et al., 1990; El-Kamel et al., 2007).
Drug delivery via sublingual route: The sublingual mucosa is generally well accepted because it is relatively permeable, gives rapid absorption, provide acceptable bioavailability of many drugs and is convenient. The sublingual route is capable of producing a rapid onset of action due to high permeability and rich blood supply which makes it appropriate for drugs with short delivery period (Squier and Wertz, 1996; Giri et al., 2010b).
Among all routes, the sublingual route is studied widely. There are two different design of sublingual dosage form, one composed of rapidly disintegrating tablets and the other consisting of soft gelatin capsules filled with liquid drug, such system before absorption to mucosa create a very high drug conc. in sublingual region (Ishida et al., 1982). Generally, sublingual route is used for drug delivery in treatment of acute disorders, but due to washing of its surface by saliva and tongue activity it makes it difficult to keep the dosage form in contact for an extended period of time with mucosa (Chiappin et al., 2007; Ryan et al., 1997).
Drug delivery via buccal route: The buccal mucosa is less permeable than sublingual area and they generally do not provide rapid absorption as sublingual administration. Buccal mucosa is more fitted for sustained and controlled delivery application, delivery of less permeable molecules and peptide drugs because of immobile mucosa. (Aungst and Rogers, 1989; Singh et al., 2011a). Both application and removal of a drug from buccal mucosal site are very convenient (Verma et al., 2011). The buccal mucosa is a useful route for the treatment of either local or systemic therapies overcoming the drawbacks of conventional administration routes. The buccal mucosa for its permeability and robustness in comparison to other mucosal tissues, is more tolerant to potential allergens and has a reduced tendency to irreversible irritation or damage. So, it has been largely investigated as a potential site for controlled drug delivery in various chronic systemic therapies (Chiappin et al., 2007).
BUCCAL ABSORPTION
Mechanism: In the oral mucosa both the hydrophilic and lipophilic regions are coexisting, for which there are two routes for drug transport, i.e., the paracellular and the transcellular routes. For hydrophilic compounds the paracellular route is the primary route, it is difficult for a hydrophilic compound to penetrate into the lipophilic cell membrane and thus, the intercellular space is the preferred route for drug transport. (Harris and Robinson, 1992; Shojaei and Li, 1997; Alur et al., 2002; Lorenza et al., 2008).
Lipophilic compounds would have low solubilities in the hydrophilic intercellular spaces and cytoplasm (Peppas and Buri, 1985).The cell membrane, although, is relatively lipophilic in nature hydrophilic solutes will have difficulty permeating through the cell membrane due to a low partition coefficient (Harris and Robinson, 1992). Some of hydrophilic macromolecular therapeutic agents like polysaccharides, oligonucleotides, peptides, can be delivered as controlled delivery via buccal mucosa. To overcome low permeability the absorption enhancer may be required which can improve bioavailability of the high molecular weight drugs (Senel and Hincal, 2001; Lu and Low, 2002).
Dynamic: The first order rate process describes oral mucosal absorption of drugs adequately. Various potential barriers have been identified as obstacles to oral mucosa drug absorption. They mainly include mucus layer, keratinized layer, intercellular lipid of epithelium, basement membrane and lamina propria. The absorptive membrane thickness, blood supply/lymph drainage cell renewal and enzyme content helps in reduction of rate and amount of drug entering the systemic circulation.
The systemic circulation pointed out that salivary secretion alters the buccal absorption kinetics from drug solution by changing the concentration of drug in the mouth. They proposed a linear relationship between salivary secretion and time thus:
dM-KC
dt ViVt
where, ‘m’ and ‘C’ are the mass and concentration of drug in mouth at time ‘t’, Vi, the volume of solution put into mouth cavity and ‘V’ is salivary secretion rate (Kumar et al., 2004).
FACTORS AFFECTING BUCCAL ABSORPTION
The oral cavity is a complex environment for drug delivery, as there are many interdependent and independent factors which reduce the absorbable concentration at the site of absorption.
Physicochemical factors affecting buccal absorption:
| • | Size: Smaller molecules (75-100 Da) generally exhibit rapid transport across the mucosa, with decreasing permeability as molecular size increases (Vaughan, 2003) |
| • | Partition coefficient: When partition coefficient increase, permeability of drug through lipoidal membrane also increase |
| • | pH: pH at the site of drug absorption can influence the partition coefficient. With increasing pH, the partition coefficient of acidic drugs decreases while that of basic drugs increases (Rao et al., 1998) |
| • | Ionization of drug: Both pKa and pH at the mucosal surface influence the ionization of a drug. Lipid solubility is exhibited appreciably only by the nonionized form of many weak acids and weak bases and thus the ability to cross lipoidal membranes (Ajazuddin, 2010) |
Physiological factors affecting buccal absorption:
| • | Inherent permeability of the epithelium |
| • | Thickness of epithelium (Swarbrick, 1999) |
| • | Blood supply |
| • | Metabolic activity |
| • | Saliva and mucus |
| • | Ability to retain delivery system |
| • | Species differences |
| • | Transport routes and mechanisms (Chatterjee, 1985) |
MUCOADHESION/BIOADHESION
Definition
Adhesion: Adhesion can be defined as the bond produced by contact between a pressure sensitive adhesive and a surface (Jimenez et al., 1993; Suryawanshi et al., 2010).
Mucoadhesion: Mucoadhesion can be defined as the phenomenon of the attachment of natural or synthetic macromolecule to mucin layer of mucosal surface or epithelial surface. (Longer and Robinson, 1986; Laura et al., 2009).
Bioadhesion: Bioadhesion is an Interfacial phenomenon in which two materials, at least one of which is biological nature are held together for extended periods of time by means of interfacial forces (Mathias and Hussain, 2010).
Stages of mucoadhesion: Dry or partially hydrated dosage form involve two basic steps in mucoadhesion shown in (Fig. 6). First step involve contact stage, where intimate contact is formed between the mucoadhesive and mucous membrane. The buccal patch is placed within the buccal cavity in contact with required mucosa and to the place to allow adhesion to occur. Second step involve consolidation stage where various physiochemical interaction occur to consolidate and strengthen the adhesive joint which prolongs adhesion (Smart, 2005; Omari et al., 2012; Patel et al., 2007a,b; Huang et al., 2000).
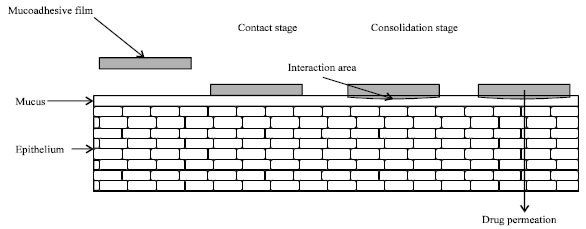 | |
| Fig. 6: | Contact and consolidation stages of mucoadhesion (Morales and McConville, 2011) |
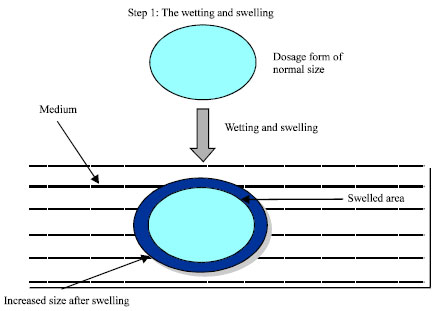 | |
| Fig. 7: | Wetting and swelling of polymer (Aidoo and Sheila, 2009) |
Mechanism of mucoadhesion: The mechanisms responsible in the formation of bioadhesive bonds are not fully known, however most research has described bioadhesive bond formation as a three step process:
| • | Step 1: Wetting and swelling of polymer |
| • | Step 2: Interpenetration between the polymer chains and the mucosal membrane (Varum et al., 2008) |
| • | Step 3: Formation of Chemical bonds between the entangled chains (Smart, 2005) |
| • | Step 1: The wetting and swelling step occurs when the polymer spreads over the surface of the biological substrate or mucosal membrane in order to develop an intimate contact with the substrate as shown in (Fig. 7) (Bhatt, 2009; Hagerstrom, 2003). Swelling of polymers occur because the components within the polymers have an affinity for water (Aidoo and Sheila, 2009) |
| • | Step 2: Glycoproteins the high molecular weight polymers composes the surface of mucosal membrane. A great area of contact shown between chains of mucoadhesive polymer and mucous gel network as shown in (Fig. 8) (Hagerstrom, 2003; Alexander et al., 2011a; Sharma et al., 2009) |
| • | Step 3: This step include entanglement and formation of weak chemical bonds along with secondary bonds between the polymer chains. Primary bonds such as covalent bond and weaker secondary interactions such as Van der Waals interactions and hydrogen bonds are formed in mucin molecules which is also showed in (Fig. 9). Strong adhesion between polymers is formed during the manufacturing of bioadhesive formulations as primary and secondary bonds are exploited (Hagerstrom, 2003; Alexander et al., 2011b; Fasina et al., 2007) |
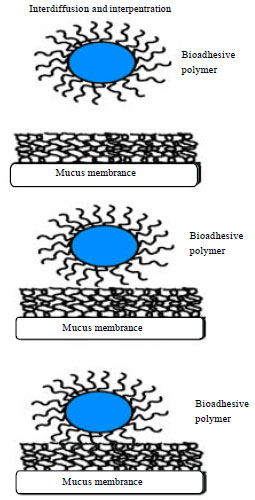 | |
| Fig. 8: | Interdiffusion and interpenetration of polymer and mucus (Smart, 2005) |
 | |
| Fig. 9: | Entanglement of Polymer and Mucus by Chemical bonds (Hagerstrom, 2003) |
Theories of mucoadhesion: Mucoadhesion is described as a complex process and various other theories are explained to describe mechanisms are known but other numerous theories should be considered as supplement of mucus/substrate interaction.
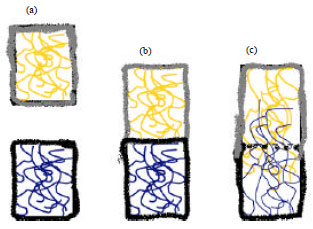 | |
| Fig. 10(a-c): | The diffusion theory of adhesion, (a) Top (polymer) layer and bottom (mucus) layer before con-tact, (b) Top layer and bottom layer immediately after contact and (c) Top layer and bottom layer after contact (Punitha and Girish, 2010) |
The diffusion theory of adhesion is shown in (Fig. 10) (Andrews et al., 2009; Alexander et al., 2011a; Sharma et al., 2011):
| • | Wettability theory |
| • | The electronic theory |
| • | The fracture theory |
| • | The adsorption theory |
| • | The diffusion-interlocking theory (Lee and Kellaway, 2000) |
FACTOR WHICH AFFECT MUCOADHESION IN ORAL CAVITY
The bioadhesive power of a polymer or of a progression of polymers is affected by the nature of the polymer and also by the nature of the surrounding media.
Polymer related factor:
| • | Molecular weight (Chen and Cyr, 1970) |
| • | Flexibility |
| • | Hydrogen bonding capacity (Peppas and Buri, 1985) |
| • | Cross linking density |
| • | Charge (Lehr et al., 1992) |
| • | Concentration of active polymer (Khairnar et al., 2009) |
| • | Hydration (Swelling) (Gu et al., 1998) |
Environmental factor (Khar et al., 1997):
| • | Applied strength |
| • | pH |
| • | Initial contact time |
Physiological variables
Mucin turnover: These molecules interact with the mucoadhesive before they have a chance to act together with the mucus layer. Mucin turnover may depend on presence of food.
Disease states: The physiochemical properties of mucus are known to adjust during disease conditions such as common cold, gastric ulcers and ulcerative colitis, bacterial and fungal infections of the female reproductive tract (Khar et al., 1997; Rejaie, 2009).
MUCOADHESIVE POLYMER USED IN ORAL CAVITY
Ideal characteristics of mucoadhesive polymer
| • | Polymer and its degradation products should be non-toxic, non-irritant and free from leachable impurities (Mishra et al., 1996) |
| • | Should have good spreadability, wetting, swelling and solubility and biodegradability properties |
| • | The polymer and its degradation products should be non-hazardous and should be non absorbable from the mucus layer (Longer and Peppas, 1981) |
| • | It should allow daily incorporation to the drug and offer no hindrance to its release (Jimenez et al., 1993) |
| • | Should not aid in development of secondary infections such as dental caries (Wise, 2000) |
Classification of mucoadhesive polymer: (Savage, 1977).
In general, adhesive polymers can be classified as synthetic vs. natural, water-soluble vs. water insoluble and charged vs. uncharged polymers (Rao et al., 2011). Examples of the recent polymers classified in these categories are listed in Table 3.
New generation of mucoadhesive polymer: In a recent mini-review current bioadhesive polymers are classified as first generation and second generation (Lee et al., 2000). Newer polymers are capable of forming covalent bonds with the mucus and the underlying cell layers and hence, exhibit improved chemical interactions (Langoth et al., 2003).
The new generation polymer are:
| • | Thiolated mucoadhesive polymers |
| • | Target-specific, lectin-mediated bioadhesive polymers |
| • | Bacterial adhesion |
| • | Mucoadhesive polymers as enzyme inhibitors and permeation enhancers |
PERMEATION ENHANCER
Substances that facilitate the permeation through buccal mucosa are referred as permeation enhancers (Chattarajee and Walker, 1995). As most of the penetration enhancers were originally designed for purposes other than absorption enhancement, The goal of designing penetration enhancers, with improved efficacy and reduced toxicity profile is possible by understanding the relationship between enhancer structure and the effect induced in the membrane and of course, the mechanism of action (Shojaei,1998). The degree of enhancement depended on a number of factors, including the characteristics of the permeant, the composition of the delivery vehicle and whether the tissue was pretreated with enhancer (Ganem-Quintanar et al., 1997b). In some cases usage of enhancers in combination has shown synergistic effect than the individual enhancers.
The efficacy of enhancer in one site is not same in the other site because of differences in cellular morphology, membrane thickness, enzymatic activity, lipid composition and potential protein interactions are structural and functional properties. Penetration enhancement to the buccal membrane is drug specific (Shojaei, 1998).
Mechanism of permeation enhancer: Mechanisms by which penetration enhancers are thought to improve mucosal absorption are as follows:
| • | By changing mucus rheology in reducing the viscosity and/or elasticity of mucus layer |
| • | By increasing fluidity of lipid bilayer |
| • | By facilitating paracellular transport |
| • | By passing the enzymetic barrier for peptides (Bernkop-Schnurch, 2005) |
| • | By accelerating the thermodynamic activity of peptide drugs |
| • | Alteration of partition coefficient is achieved by increasing the solubility of drug via some enhancer which leads to better absorption with increased thermodynamic activity (Rathbone and Tucker, 1993) |
| • | By acting on the components at tight junctions (Siegel and Gordon, 1985) |
| Table 3: | Comparative study of buccal patch and buccal tablet |
 | |
Categories of permeation enhancer
The categories and examples of various permeation enhancers:
| • | Bile salts: sodium glycocholate, sodium deoxycholate, sodium taurocholate, sodium glycodeoxycholate, sodium taurodeoxycholate. sodium taurocholate |
| • | Chelators: Disodium EDTA, citric acid, sodium salicylate, methoxy salicylates (Kurosaki et al., 1989; Pramod and Lingappa, 2008) |
| • | Surfactants: Sodium lauryl sulfate, polyoxyethylene, Polyoxyethylene-9-laurylether, Polyoxythylene-20-cetyl ether, Benzalkonium chloride, 23-lauryl ether, cetylpyridinium chloride, cetyl trimethyl ammonium bromide (Aungst, 1994) |
| • | Non-surfactants: Unsaturated cyclic urea |
| • | Steroidal surfactants: Sodium cholate |
| • | Fatty acids: Oleic acid, capric acid, lauric acid, propylene glycol, cod liver oil methyl oleate, lysophosphatidylcholine, phosphatidylcholine (Hinton et al., 2009) |
| • | Inclusion complexes: Cyclodextrins |
| • | Thiolated polymers: Chitosan-4-thiobutylamide, chitosan- 4-thiobutylamide/GSH, chitosan-cysteine, Poly (acrylic acid)-homocysteine, polycarbophil-cysteine, polycarbophil- cysteine/GSH, chitosan-4-thioethylamide/GSH, chitosan-4-thioglycolic acid |
| • | Others: Aprotinin, azone, cyclodextrin, dextran sulfate, menthol, polysorbate 80, sulfoxides and various alkyl glycosides (Zhang et al., 1994; Chen et al., 2011) |
Buccal formulation: In the past decades, different drug delivery systems intended for buccal administration have been developed, The size of the delivery system varies with the type of formulation, i.e., a buccal tablet may be approximately 5-8 mm in diameter, whereas a flexible buccal patch may be as large as 10-15 cm2 in area. Mucoadhesive buccal patches with a surface area of 1-3 cm2 are most acceptable. Comparative study of buccal patch and buccal tablet are shown in (Table 4). It has been estimated that the total amount of drug that can be delivered across the buccal mucosa from a 2 cm2 system in 1 day is approximately 10-20 mg (Rathbone et al., 1996; Choudhary et al., 2010).
Matrix tablets/Bioadhesive buccal tablets: Monolithic tablets in their simplest version consist of a mixture of drug with a swelling bioadhesive/sustained release polymer with a bidirectional release. They can be coated on the outer or on all sides but one face with water impermeable hydrophobic substances to allow an unidirectional drug release for systemic delivery (Rathbone et al., 1996; Bose et al., 2011). In case of bilayered tablets, drug can be incorporated in the adhesive layer which comes in contact with the mucosal surface. This drug containing mucoadhesive layer is then protected from the oral cavity environment by a second upper inert layer which faces into the oral cavity. Alternatively, the drug can be incorporated into the upper non adhesive layer to release the drug into the oral cavity. Various types of matrix tablets shown in (Fig. 11) (Gupta et al., 2010; Chandira et al., 2009).
Semisolid preparations (ointments and gels): Solid dosage adhesive forms are used widely than bioadhesive gels or ointments, because they are most used for localized drug therapy within oral cavity. “ ORABASE” the original oral mucosal adhesive delivery system consist of finely ground pectin, gelatin and sodium carboxymethyl cellulose dispersed in a poly (ethylene) and a mineral oil gel base. It can be maintained at the site of application for 15-150 min.
Powders: Yamamoto et al. (2001) described a hydroxypropyl cellulose and beclomethasone-diproprionate containing powder that was sprayed onto the oral mucosa of rats. A significant increase in the residence time relative to an oral solution was seen and 2.5% of beclomethasone was retained on buccal mucosa for over 4 h (Senel and Hincal, 2001; Ch’Ng et al., 1985; Kaur and Kaur, 2011).
| Table 4: | Classification of polymers used in formulation of buccal patch (Savage, 1977) |
 | |
Buccal patches: The drawbacks of other dosage form are overcomed by development of flexible adhesive patches. Transmucosal delivery patches include unique characteristic like rapid onset of drug delivery, sustained drug release and rapid decline in the serum drug when the patch is removed. The less inter and intraindividual variability absorption profile is showed by a buccal patch which it confined to the buccal area over which it is attached.
 | |
| Fig. 11(a-f): | Schematic representation of different matrix tablets for buccal delivery. Arrows indicate the direction of drug release (Rossi et al., 2005) |
List of commercial buccal patches for oral mucosal drug delivery are shown in (Table 5). In general patches with a dissolvable matrix, patches with a non-dissolvable backing and patches with a dissolved backing are the 3 categories for classification of oral mucosal patches (Dixit and Puthli, 2009; Alagusundaram et al., 2009).
Patches with a dissolvable matrix shown in Fig. 12 are designed to release drug into the oral cavity. The mucoadhesive layer (either in drug matrix or attached to drug matrix) would prolong the duration of drug matrix in the oral cavity. Hence, in comparison to other dosage forms, these systems are longer acting and can potentially deliver more drug quantities. Patches with non-dissolvable backing shown in Fig. 13 are usually designed for systemic delivery. Since, they are closed systems and the formulations are protected from saliva, the drug concentrations are controlled and drug is continuously delivered for 10-15 h. The system include disadvantages as removal of backing by the patient after drug administration and use of only a small area. The entire patch get dissolved in oral cavity which have dissolvable backing. But these patches show shorter acting as compared to non-dissolvable backing membrane. Basically buccal patch consist of drug substance, bioadhesive polymer, plasticizers, backing membrane and permeation enhancer.
| Fig. 12: | Buccal patch with a dissolvable matrix (Veillard et al., 1987) |
| Fig. 13: | Buccal patch with a non dissolvable backing (Kurosaki et al., 1989) |
| Table 5: | List of commercial buccal patches for oral mucosal drug delivery |
 | |
| Table 6: | List of active pharmaceutical ingredients (Drugs) and polymer used in buccal patches |
 | |
The commonly used materials in backing membrane include carbopol, magnesium stearate, HPMC, HPC, CMC, polycarbophil etc. List of active pharmaceutical ingredients (Drugs) and polymer used in buccal patches are shown in Table 6. (Santos et al., 1999; Satyabrata et al., 2010; Ritthidej et al., 2002; Kumar et al., 2010).
Innovative drug delivery systems: Innovative drug delivery systems, such as lipophilic gel, buccal spray and phospholipid vesicles have been recently proposed to deliver peptides via the buccal route (Lee et al., 2000; Senel et al., 2000). A novel liquid aerosol formulation has been recently developed and it is now in clinical phase II trials.
| Table 7: | Patents on buccal patches |
 | |
This system allows precise insulin dose delivery via a metered dose inhaler in the form of fine aerosolized droplets directed into the mouth. Levels of drug in the mouth are dramatically increased compared with conventional technology. This oral aerosol formulation is rapidly absorbed through the buccal mucosal epithelium and it provides the plasma insulin levels necessary to control postprandial glucose rise in diabetic patients (Modi et al., 2002). A number of advantages are included in this novel, pain free oral insulin formulation which also show rapid absorption, precise dosing control, a simple administration technique and bolus delivery of drug. The recently devised element for delivery of insulin in buccal cavity are phospholipids, deformable vesicles and transferosomes. These vesicles are prepared from surfactants, such as sodium cholate or sodium deoxycholate. They are similar to liposomes morphologically but they pecularly respond to external stresses and their rapid shape transformation require low energy (Yang et al., 2002; Khanna et al., 1996).
Recent invention in field of buccal patches: Lots of work had been done in the field of bioadhesive drug delivery systems and the innovators had successfully patented their work with new modified systems. Some of the patents on this drug delivery have been reported in (Table 7) (Kim et al., 2011).
CONCLUSION
The ease of access and avoidance of the hepatic metabolism enable buccal drug delivery for being a potential alternative conventional oral drug delivery and parental administration which suffer from certain limitations. Almost 80% of the current commercially available formulations are limited to tablet. Oral buccal dosage forms will continue to be an exciting research focus for improving drug absorption especially for the new generation of the so called ‘biologics’, however, the palatability, irritancy and formulation retention at the site of application need to be considered during design of such formulation.
This article presents a summary of the investigations conducted by various researchers to explore the possibility of utilizing buccal drug delivery and their observations during last two to three decades. The authors expect that this article can be useful and ready reference to those who shall be interested to design, develop a buccal drug delivery system.
ACKNOWLEDGMENT
The authors would like to acknowledge the assistance provided by the Management of Rugnta College of Pharmaceutical Sciences and Research, Kohka Road, Bhiali, C.G. (India) for collection of literatures.
ABBREVIATION
| MCG | = | Membrane coating granules |
| cm | = | Centimeter |
| m | = | Mass |
| C | = | Concentration |
| t | = | Time |
| V | = | Volume |
| Da | = | Dalton |
| L | = | Litre |
| mm | = | Millimeter |
| mg | = | Milligram |
| E | = | Young’s modules of elasticity |
| ε | = | Fracture energy |
| L | = | Critical crack length |
| cal | = | Calorie |
| K | = | Kilo |
| EDTA | = | Ethylenediaminetetraacetic acid |
| h | = | Hour |
| kg | = | Kilogram |
| RH | = | Relative humidity |
| Wvt | = | Wvt |
| S | = | Surface area |
| rpm | = | Resolution per min |
| NK | = | Non- keratinized |
| K | = | Keratinized |
| SD | = | Standard deviation |
| HPMC | = | Hydroxy propyl methylcellulose |
| HPC | = | Hydroxy propyl cellulose |
| CMC | = | Carboxymethylcellulose |
| PVA | = | Polyvinylalcohol |
| PVP | = | Polyvinylpyrrolidone |
| CP | = | Carbopol |
| PEG | = | Polyethylene glycol |
| EC | = | Ethyl cellulose |
| HEC | = | Hydroxyethylcellulose |
| US | = | United state |
| cps | = | Centipoises |
| PC | = | Polycarbonate |
| DEAE | = | Diethylaminoethyl cellulose |
| TMC | = | Trimethylcellulose |
| PAA | = | Polyacrylic acid |
| CP | = | Conductive polymer |
REFERENCES
- Abdollahi, M., A. Bahreini-Moghadam, B. Emami, F. Fooladian and K. Zafari, 2003. Increasing intracellular cAMP and cGMP inhibits cadmium-induced oxidative stress in rat submandibular saliva. Comp. Biochem. Physiol. C. Toxicol. Pharmacol., 135: 331-336.
CrossRefDirect Link - Ahmed, Y.A.E.G., G. Kmel and A.A.E.M. Ahmad, 2011. Histomorphological studies on the stomach of the japanese quail. Asian J. Poult. Sci., 5: 56-67.
CrossRefDirect Link - Akhionbare, O. and P.I. Ojehanon, 2007. The palliative effects of lidocaine with adrenaline on Recurrent Aphthous Stomatitis (RAS). J. Medical Sci., 7: 860-864.
CrossRefDirect Link - Alagusundaram, M., B. Chengaiah, S. Ramkanth, S.A. Parameswari, C.M.S. Chetty and D. Dhachinamoorthi, 2009. Formulation and evaluation of Mucoadhesive buccal films of ranitidine. Int. J. Pharm. Tech. Res., 1: 557-563.
Direct Link - Alexander, A., Ajazuddin, D.K. Tripathi, T. Verma, Swarna, J. Maurya and S. Patel, 2011. Mechanism responsible for mucoadhesion of mucoadhesive drug delivery system: A review. Int. J. Applied Biol. Pharm. Technol., 2: 434-445.
Direct Link - Alexander, A., M. Ajazuddin, M. Swarna, M. Sharma and D.K. Tripathi, 2011. Polymers and permeation enhancers: Specialized components of mucoadhesives. Stamford J. Pharm. Sci., 4: 91-95.
CrossRefDirect Link - Allen, A., D.A. Hutton, J.P. Pearson and L.A. Sellars, 1984. Mucus glycoprotein, structure, gel formation and gastrointestinal mucus function, mucus and mucosa. Ciba Found. Symp., 109: 137-156.
PubMedDirect Link - Amarji, B., Ajazuddin, D. Raghuwanshi, S.P. Vyas and P. Kanaujia, 2007. Lipid Nano Spheres (LNSs) for enhanced oral bioavailability of amphotericin B: Development and characterization. J. Biomed. Nanotechnol., 3: 264-269.
Direct Link - Andrews, G.P., T.P. Laverty and D.S. Jones, 2009. Mucoadhesive polymeric platforms for controlled drug delivery. Eur. J. Pharm. Biopharm., 71: 505-518.
CrossRefPubMedDirect Link - Arya, R.K., H. Chaurasia, P. Bharadwaj, N. Garud, and S. Palani, 2011. Development and evaluation of mucoadhesive buccal tablet of salbutamol sulphate. Int. Res. J. Pharm., 2: 159-162.
Direct Link - Aungst, B.J. and N.J. Rogers, 1989. Comparison of the effects of various transmucosal absorption promoters on buccal insulin delivery. Int. J. Pharm., 53: 227-235.
CrossRef - Al-Bassiouny, A.M.M.E., 2009. Posterior pillar flap palatoplasty: A new surgical technique for treatment of snoring: Initial experience. J. Med. Sci., 9: 118-125.
CrossRefDirect Link - Basu, B., K. Garala and J. Thimmasetty, 2010. Formulation and evaluation of pimozide buccal mucoadhesive patches. Int. J. Pharm. Sci. Nanotech., 2: 739-748.
Direct Link - Bernkop-Schnurch, A., 2005. Mucoadhesive systems in oral drug delivery. Drug Discov. Today Technol., 2: 83-87.
Direct Link - Bhyan, B., S. Jangra, M. Kaur and H. Singh, 2011. Orally fast dissolving film: Innovations in formulation and technology. Int. J. Pharm. Sci. Rev. Res., 9: 50-57.
Direct Link - Bose, P.C.S., S. Reddy, P. Sarithad and R. Nagaraju, 2011. Design and evaluation of buccal mucoadhesive patches containing oxybutynin HCL. Res. J. Pharm. Biol. Chem. Sci., 3: 1015-1024.
Direct Link - Chandira, M., Mehul, Debjit, Chiranjib, Kumudhavalli and B. Jayakar, 2009. Formulation, design and development of buccoadheshive tablets of verapamil hydrochloride. Int. J. PharmTech. Res., 1: 1663-1677.
Direct Link - Chen, Y., H. Zhang, H. Wang and H. Yang, 2011. Effect of diatery addition of non-ionic surfectants on ruminal metabolism and nutrient digestion of chinese merino sheep. Asian J. Anim. Vet. Adv., 6: 688-696.
Direct Link - Chiappin, S., G. Antonelli, R. Gatti and E.F. De Palo, 2007. Saliva specimen: A new laboratory tool for diagnostic and basic investigation. Clin. Chim. Acta, 383: 30-40.
PubMedDirect Link - Collins, A.E.M., P.B. Deasy, D.J.M. Carthy and D.B. Shanley, 1989. Evaluation of a controlled release compact containing tetracycline hydrochloride bonded to tooth for the treatment of periodontal disease. Int. J. Pharm., 51: 103-114.
Direct Link - Collins, L.M.C. and C. Dawes, 1987. The surface area of adult human mouth and thickness of salivary film covering the teeth and Oral mucosa. J. Dent. Res., 66: 1300-1302.
Direct Link - Dawes, C., 2007. Gland size estimation and body mass index improve salivary flow rate assessment. Arch. Oral Biol., 52: 409-410.
PubMedDirect Link - Dharani, S. and Shayeda, 2010. Formulation and in vitro evaluation of mucoadhesive buccal patches of ondansetron hydrochloride. Int. J. Pharm. Sci. Nanotech., Vol. 3.
Direct Link - Dixit, R.P. and S.P. Puthli, 2009. Oral strip technology: Overview and future potential. J. Control Release, 139: 94-107.
Direct Link - Edgar, W.M., 1990. Saliva and dental health. Clinical implications of saliva: Report of a consensus meeting. Br. Dent. J., 169: 96-98.
PubMedDirect Link - Elkayam, R., M. Friedman, A. Stabholz, A.W. Soskolne, M.N. Sela and L. Golub, 1988. Sustained release device containing minocycline for local treatment of periodontal disease. J. Control. Rel., 7: 231-236.
Direct Link - Fasina, Y.O., E.T. Moran, C.M. Ashwell, D.E. Conner, M. Leslie and S.R. Mckee, 2007. Effect of dietary gelatin supplimetation on the expression of selected enterocyte genes, intestinal development and early chick performance. Int. J. Poult. Sci., 6: 944-951.
Direct Link - Galati, G., S. Teng, M.Y. Moridani, T.S. Chan and P.J. O'Brien, 2000. Cancer chemoprevention and apoptosis mechanisms induced by dietary polyphenolics. Drug Metab. Drug Interact., 17: 311-349.
PubMedDirect Link - Galey, W.R., H.K. Lonsdale and S. Nacht, 1976. The in vitro permeability of skin and Buccal mucosa to selected drugs and tritiated water. J. Invest. Dermat., 67: 713-717.
CrossRefDirect Link - Gandhi, R.B. and J.R. Robinson, 1994. Oral cavity as a site for bioadhesive drug delivery. Adv. Drug Deliv. Rev., 13: 43-74.
Direct Link - Gandhi, R.B. and J.R. Robinson, 1988. Bioadhesion in drug delivery. Ind. J. Pharm. Sci., 50: 145-152.
Direct Link - Ganem-Quintanar, A., F. Rieg and P. Buri, 1997. Contribution of lipid components to the permeability barrier of Oral mucosa. Eur. J. Pharm. Biopharm., 44: 107-120.
Direct Link - Ganem-Quintanar, A., Y.N. Kalia, F. Falson-Rieg and P. Buri, 1997. Mechanism of oral permeation enhancement. Int. J. Pharm., 156: 127-142.
Direct Link - Giradkar, M.A., A.D. Channawar, E. Kajale, R.S. Sridhar, B.V. Kamble, B.V. Bakde and A.V. Chandewar, 2010. Chandewar. design, development and in vitro evaluation of bioadhesive dosage form for buccal route. Int. J. Pharm. Res. Dev., 2: 1-20.
Direct Link - Ritthidej, G.C., T. Phaechamud and T. Koizumi, 2002. Moist heart treatment on physicochemical change of chitosan salt films. Int. J. Pharm., 232: 11-22.
PubMed - Giri, T.K., H. Badwaik, A. Alexander and D.K. Tripathi, 2010. Solubility enhancement of ibuprofen in the presence of hydrophilic polymer and surfactant. Int. J. Applied Biol. Pharm. Technol., 1: 793-800.
Direct Link - Gu, J.M., J.R. Robinson and S.H. Leung, 1998. Binding of acrylic polymers to mucin/epithelial surfaces: Structure-property relationships. Crit. Rev. Ther. Drug Carr. Syst., 5: 21-67.
PubMedDirect Link - Gupta, V., S.K. Shukla, S.M. Shrivastava, S. Shukla and K. Kumar et al., 2010. Studies of in vitro evaluation and formulation of aceclofenac loaded PLGA microspheres. Int. J. Pharmacol., 6: 726-731.
CrossRefDirect Link - Gupta, S.K., I.J. Singhvi, M. Shirsat, G.Karwani, A. Agarwal and A. Agarwal, 2011. Buccal adhesive drug delivery system: A review. Asian J. Biochem. Pharm. Res., 1: 105-114.
Direct Link - Hakan, U., S. Naldoken, M.T. Ercan, N. Ulutuncel and K. Araz, 1990. Blood flow to palatal mucosal and skin grafts in mandibular labial vestibuloplasty measured by 133Xe clearance technique. J. Isl. Acad. Sci., 3: 74-77.
Direct Link - El-Kamel, A.H., L.Y. Ashri and I.A. Alsarra, 2007. Micromatricial metronidazole benzoate film as a local mucoadhesive delivery system for treatment of periodontal diseases. AAPS Pharm. Sci. Tech., Vol. 8.
CrossRefDirect Link - Herrera, J.L., M.F. Lyons and L.F. Johnson, 1988. Saliva: Its role in health and disease. J. Clin. Gastroenterol., 10: 569-578.
PubMedDirect Link - Hinton, Jr. A., J.A. Cason, R.J. Buhr and K. Liljebjelke, 2009. Bacteria recovered from whole-carcass rinsates of broiler carcasses washed in a spray cabinet with lauric acid-potassium hydroxide. Int. J. Poult. Sci., 8: 1022-1027.
CrossRefDirect Link - Houghton, A.R., 2002. Angiotensin II receptor antagonists in chronic heart failure: Where do they fit? Drugs, 62: 1433-1440.
PubMedDirect Link - Ch'Ng, H.S., H. Park, P. Kelly and J.R. Robinson, 1985. Bioadhesive polymers as platforms for oral controlled drug delivery-II: Synthesis and evaluation of some swelling water-insoluble bioadhesive polymers. J. Pharm. Sci., 74: 399-405.
PubMedDirect Link - Huang, Y., W. Leobandung, A. Foss and N.A. Peppas, 2000. Molecular aspects of muco and bioadhesion: tethered structures and site-specific surfaces. J. Control Release., 65: 63-71.
Direct Link - Ishida, M., N. Nambu and T. Nagai, 1982. Mucosal dosage form of lidocaine for toothache using hydroxypropyl cellulose and carbopol. Chem. Pharm. Bull., 30: 980-984.
PubMedDirect Link - Jessie, K., O.H. Hashim and Z.H.A. Rahim, 2008. Protein precipitation method for salivary proteins and rehydration buffer for two-dimensional electrophoresis. Biotechnology, 7: 686-693.
CrossRefDirect Link - Jug, M., M. Becirevic-Lacan and S. Bengez, 2009. Novel cyclodextrin-based film formulation intended for buccal delivery of atenolol. Drug Dev. Ind. Pharm., 35: 796-807.
PubMedDirect Link - Kaur, A. and G. Kaur, 2011. Mucoadhesive buccal patches based on interpolymer complexes of chitosan-pectin for delivery of carvedilol. Saudi Pharm. J., 20: 21-27.
Direct Link - Khairnar, A., P. Jain, D. Baviskar and D. Jain, 2009. Developmement of mucoadhesive buccal patch containing aceclofenac: In vitro evaluations. Int. J. PharmTech Res., 1: 978-981.
Direct Link - Khanna, R., S.P. Agarwal and A. Ahuja, 1996. Preparation and evaluation of bioerodible bucal tablet containing clotrimazole. Int. J. Pharm., 138: 67-73.
CrossRefDirect Link - Langoth, N., J. Kalbe and A. Bernkop-Schnurch, 2003. Development of buccal drug delivery systems based on a thiolated polymer. Int. J. Pharm., 25: 141-148.
Direct Link - Laura, S., J. Domenechc and N. Peppasa, 2009. Engineering design and molecular dynamics of mucoadhesive drug delivery systems as targeting agents. Eur. J. Pharm. Biopharm., 71: 519-528.
CrossRefDirect Link - Lee, J. and I.W. Kellaway, 2000. Buccal permeation of [d-Ala2, d-Leu5]enkephalin from liquid crystalline phases of glyceryl monooleate. Int. J. Pharm., 195: 35-38.
Direct Link - Lee, J.W., J.H. Park and J.R. Robinson, 2000. Bioadhesive-based dosage forms: The next generation. J. Pharm. Sci., 89: 850-866.
CrossRefDirect Link - Lehr, C.M., J.A. Bouwstra, E.H. Schacht and H.E. Junginger, 1992. In vitro evaluation of mucoadhesive properties of chitosan and some other natural polymers. Int. J. Pharm., 78: 43-48.
Direct Link - Llena-Puy, C., 2006. The role of saliva in maintaining oral health and as an aid to diagnosis. Med. Oral Patol. Oral Cir. Bucal., 11: E449-E455.
PubMed - Longer, R.S. and N.A. Peppas, 1981. Present and future applications of biomaterials in controlled drug delivery systems. Biomaterials, 2: 201-214.
PubMedDirect Link - Lorenza, G.M., H. Sandra and V. Jeesus, 2008. Inventions designed to enhance drug delivery across pithelial and endothelial cells through the paracellular pathways. Recent. Adv. Drug Deliv. Formul., 2: 145-176.
PubMedDirect Link - Lu, Y. and P.S. Low, 2002. Folate-mediated delivery of macromolecular anticancer therapeutic agents. Adv. Drug Deliv. Rev., 54: 675-693.
PubMedDirect Link - Malekipour, M.R., M. Messripour and F. Shirani, 2008. Buffering capacity of saliva in patients with active dental caries. Asian J. Biochem., 5: 280-283.
CrossRefDirect Link - Mathias, N.R. and M.A. Hussain, 2010. Non-invasive systemic drug delivery: Developability considerations for alternate routes of administration. J. Pharm. Sci., 99: 1-20.
Direct Link - Repka, M.A., K. Gutta, S. Prodduturi, M. Munjal and S.P. Stodghill, 2005. Characterization of cellulosic hot-melt extruded films containing lidocaine. Eur. J. Pharm. Biopharm., 59: 189-196.
Direct Link - Modi, P., M. Mihic and A. Lewin, 2002. The evolving role of oral insulin in the treatment of diabetes using a novel RapidMistTM system. Diabetes Metab. Res. Rev., 18: S38-S42.
CrossRefDirect Link - Jafar, M. and S. Ali, 2011. Development and evaluation of Meloxicam solid dispersion loaded buccal patches. J. Applied Pharm. Sci., 1: 77-82.
Direct Link - Morales, J.O. and J.T. McConville, 2011. Manufacturing and characterization of mucoadhesive buccal films. Eur. J. Pharm. Biopharmaceut., 77: 187-199.
CrossRef - Thomas, C. and M.Y. Moridani, 2010. Interindividual variations in the efficacy and toxicity of vaccines. Toxicology, 278: 204-210.
CrossRef - Omari, S.M.S., N.G.H.A. Al-Rob, S.M. Salhimi, A.F.A. Aisha and S.M.N. Khasib et al., 2012. Comparative phosphorylation profiles of focal adhesion kinase among cancer colon cell lines and tissues. Am. J. Biochem. Mol. Biol., 2: 146-156.
CrossRefDirect Link - Pajoumand, A., N. Jalali, M. Abdollahi and S. Shadnia, 2003. Successful treatment of acetaminophen overdose associated with hepatic failure. Hum. Exp. Toxicol., 22: 453-458.
PubMed - Parmar, H.G., J.J. Jain, T.K. Patel and V.M. Patel, 2010. Buccal patch: A technical note. Int. J. Pharm. Sci. Rev. Res., 4: 178-182.
Direct Link - Patel, A.R., D.A. Patel and S.V. Chaudhry, 2011. Mucoadhesive buccal drug delivery system. Int. J. Pharm. Life Sci., 2: 848-856.
Direct Link - Patel, K.V., N.D. Patel, H.D. Dodiya and P.K. Shelat, 2011. Buccal bioadhesive drug delivery system: An overview. Int. J. Pharm. Biol. Arch., 2: 600-609.
Direct Link - Patel, R.S. and S.S. Poddar, 2009. Development and characterization of mucoadhesive buccal patches of salbutamol sulphate. Curr. Drug Deliv., 6: 140-144.
PubMedDirect Link - Patel, V.F., F. Liu and M.B. Brown, 2001. Advances in oral transmucosal drug delivery. J. Control. Release, 153: 106-116.
PubMed - Peppas, N.A. and P.A. Buri, 1985. Surface, interfacial and molecular aspects of polymer bioadhesion on soft tissues. J. Control. Rel., 2: 257-275.
CrossRefDirect Link - Pourhashemi, S.J., M.G. Motlagh and G.R.J. Khaniki, 2007. Prevalence and intensity of gingivitis among 6-10 Years Old elementary school children in Tehran, Iran. J. Medical Sci., 7: 830-834.
CrossRefDirect Link - Pramod, T. and K. Lingappa, 2008. Immobilization of Aspergillus niger in polyurethane foam for citric acid production from carob pod extract. Am. J. Food Technol., 3: 252-256.
CrossRefDirect Link - Punitha, S. and Y. Girish, 2010. Polymers in mucoadhesive buccal drug delivery system-A review. Int. J. Res. Pharm. Sci., 1: 170-186.
Direct Link - Qureshi, T.A., K.B. Mirbahar, M.U. Samo, N.M. Soomro, A.A. Solangi and A. Memon, 2006. Clinical study of experimentally induced anaphylactic shock in goats. Int. J. Pharmacol., 2: 357-361.
CrossRefDirect Link - Rathbone, M.J., B.K. Drummond and I.G. Tucker, 1994. Oral cavity as a site for systemic drug delivery. Adv. Drug Delivery Rev., 13: 1-22.
CrossRefDirect Link - Riikka L., E. Suihko, K. Toukola and M. Bjorkqvist, 2009. Intraorally fast dissolving particles of a poorly soluble drug: Preparation and in vitro characterization. Eur. J. Pharmaceut. Biopharm., 71: 271-281.
PubMed - Rohaya, M.A.W., S. Sahidan, Z.A. Zaidah, H. Fahrul Zaman, A.W. Nuraliza and Z.A.S. Hisham, 2010. Stability of human salivary lactate dehydrogenase in the present of ethylenediaminetetraacetic acid, glycerol and polyethylene glycol at various temperatures: Preliminary study. J. Biol. Sci., 10: 520-525.
CrossRefDirect Link - Rossi, S., G. Sandri and C.M. Caramella, 2005. Buccal drug delivery: A challenge already won? Drug Discovery Today: Technol., 2: 59-65.
CrossRefDirect Link - Rraju, K.N., S. Velmurugan, B. Deepika and S. Vinushitha, 2011. Formulation and in vitro evaluation of buccal tablets of metoprolol tartrate. Int. J. Pharm. Pharm. Sci., 3: 239-246.
Direct Link - Ryan, R., A. Elkind, C.C. Baker, W. Mullican, S. DeBussey and M. Asgharnejad, 1997. Sumatriptan nasal spray for the acute treatment of migraine: Results of two clinical studies. Neurology, 49: 1225-1230.
Direct Link - Samaranayake, L. and M. Ferguson, 1994. Delivery of antifungal agents to the oral cavity. Adv. Drug Delivey Rev., 13: 161-179.
CrossRefDirect Link - Sangeetha, S., D.N. Venkatesh, P.N. Krishan and R. Saraswathi, 2010. Mucosa as a route for systemic drug delivery. Res. J. Pharmaceut. Biol. Chem. Sci., 1: 178-187.
Direct Link - Santos, C.A., J.S. Jacob, B.A. Hertzog, B.D. Freedman, D.L. Press, P. Harnpicharnchai and E. Mathiowitz, 1999. Correlation of two bioadhesion assays: The everted sac technique and the CAHN microbalance. J. Control Release, 61: 113-122.
CrossRefDirect Link - Satyabrata, B., P. Ellaiah, R. Choudhury, K.V.R. Murthy, P. Bibhutibhusan and M.S. Kumar, 2010. Design and evaluation of methotrexate buccal mucoadhesive patches. Int. J. Pharm. Biomed. Sci., 1: 31-36.
Direct Link - Savage, D.C., 1977. Microbial ecology of the gastrointestinal tract. Annu. Rev. Microbiol., 31: 107-133.
CrossRefPubMedDirect Link - Scholz, O.A., A. Wolff, A. Schumacher, I. Libero, G.G. Campisi, T. Ciach and T. Velten, 2008. Drug delivery from the oral cavity: focus on a novel mechatronic delivery device. Drug Discovery Today, 13: 247-253.
Direct Link - Senel, S., M.J. Kremer, S. Kas, P.W. Wertz, A.A. Hincal and C.A. Squier, 2000. Enhancing effect of chitosan on peptide drug delivery across buccal mucosa. Biomaterials, 21: 2067-2071.
PubMed - Senel, S. and A.A. Hincal, 2001. Drug permeation enhancement via buccal route: Possibilities and limitations. J. Controlled Release, 72: 133-144.
CrossRef - Shakya, P., N.V.S. Madhav, A.K. Shakya and K. Singh, 2011. Palatal mucosa as a route for systemic drug delivery: A review. J. Control Rel., 151: 2-9.
Direct Link - Shanker, G., C.K. Kumar, C.S.R. Gonugunta, B.V. Kumar and P.R. Veerareddy, 2009. Formulation and evaluation of bioadhesive buccal drug delivery of tizanidine hydrochloride tablets. AAPS PharmSciTech, 10: 530-539.
CrossRefPubMedDirect Link - Sharma, S., Swarna, K.M.J. Ajazuddin and A. Alexander, 2011. Theories and factor affecting mucoadhesive drug delivery system: A review. Int. J. Res. Ayur. Pharma., 2: 1155-1161.
Direct Link - Shojaei, A.H., 1998. Buccal mucosa as a route for systemic drug delivery: A review. J. Pharm. Pharmaceut. Sci., 1: 15-30.
PubMedDirect Link - Siegel, J.A. and H.P. Gordon, 1985. Effects of surfactants on the permeability of canine oral mucosa in vitro. Toxicol. Lett., 26: 153-157.
CrossRefPubMedDirect Link - Singh, M.R., D. Singh and S. Saraf, 2011. Formulation optimization of controlled delivery system for antihypertensive peptide using response surface methodology. Am. J. Drug Discovery Dev., 1: 174-187.
CrossRef - Slomiany, B.L., V.L.N. Murty, J. Piotrowski and A. Slomiany, 1996. Salivary mucins in oral mucosal defense. Gen. Pharmacol. Vascular Syst., 27: 6761-6771.
PubMedDirect Link - Smart, J.D., 2004. Lectin mediated drug delivery in the oral cavity. Adv. Drug Del. Rev., 56: 481-489.
Direct Link - Smart, J.D., 2005. The basics and underlying mechanisms of mucoadhesion. Adv. Drug Deliv. Re., 57: 1556-1568.
Direct Link - Squier, C.A. and P.W. Wertz, 1993. Permeability and the pathophysiology of oral mucosa. Adv. Drug Deliv. Rev., 12: 13-24.
Direct Link - Squier, C.A., P. Cox and P.W. Wertz, 1991. Lipid content and water permeability of skin and oral mucosa. J. Invest. Dermat., 96: 123-126.
PubMedDirect Link - Steven, J.R.J.M., 2002. Transmucosal delivery of testosterone in rabbits using novel bi-layer Mucoadhesive Wax-film composite disks. Pharm. Res., 91: 2016-2025.
PubMedDirect Link - Sudhakar, Y., K. Kuotsu and A.K. Bandyopadhyay, 2006. Buccal bioadhesive drug delivery-a promising option for orally less efficient drugs. J. Control. Release, 114: 15-40.
CrossRefPubMedDirect Link - Humphrey, S.P. and R.T. Williamson, 2001. A review of saliva: normal composition, flow and function. J. Prosthet Dent., 85: 162-169.
CrossRef - Tabak, L.A., M.J. Levine, I.D. Mandel and S.A. Ellison, 1982. Role of salivary mucins in the protection of the oral cavity. J. Oral Pathol., 11: 1-17.
PubMedDirect Link - Taliyan, R. and P.L. Sharma, 2010. Diabetic neuropathic pain: An update and novel pharmacological strategies for relief of pain. J. Med. Sci., 10: 93-109.
CrossRefDirect Link - Tayal, S. and N. Jain, 2011. Buccal control drug delivery system: A review. Int. J. Pharm. Sci. Res., 2: 13-24.
Direct Link - Trivedi, N.D., U.N. Trivedi, M.M. Patel, J.K. Patel and A. Bhandari, 2011. Preparation and evaluation of floating matrix tablet of ranitidine. Am. J. Drug Discovery Dev., 1: 8-23.
CrossRefDirect Link - Vamshi, Y.V., K. Chandrasekhar, G. Ramesh and Y.M. Rao, 2007. Development of mucoadhesive patches for buccal administration of carvedilol. Curr. Drug Del., 4: 27-29.
Direct Link - Varshosaz, J., F. Jaffari and S. Karimzadeh, 2006. Development of bioadhesive chitosan gels for topical delivery of lidocaine. Sci. Pharm., 74: 209-223.
Direct Link - Varum, F.J., E.L. McConnell, J.J. Sousa, F. Veiga and A.W. Basit, 2008. Mucoadhesion and the gastrointestinal tract. Crit. Rev. Ther. Drug Carrier Syst., 25: 207-258.
PubMedDirect Link - Veillard, M.M., M.A. Longer, T.W. Martens and J.R. Robinson, 1987. Preliminary studies of oral mucosal delivery of peptide drugs. J. Controlled Release, 6: 123-131.
CrossRefDirect Link - Veuillez, F., Y.N. Kalia, Y. Jacques, J. Deshusses and P. Buri, 2001. Factors and strategies for improving buccal absorption of peptides. Eur. J. Pharm. Biopharm., 51: 93-109.
PubMed - Verma, N., A.K. Ghosh and P. Chattopadhyay, 2011. Preparation and evaluation of mucoadhesive buccal patches containing metoprolol succinate. Int. J. Pharm. Sci., 3: 1075-1078.
Direct Link - De Vries, M.E., H.E. Bodde, J.C. Verhoef and H.E. Junginger, 1991. Developments in buccal drug delivery. Crit. Dev. Ther. Drug Carrier Syst., 8: 271-303.
PubMed - Wertz, P.W. and C.A. Squier, 1991. Cellular and molecular basis of barrier function in oral epithelium. Crit. Rev. Ther. Drug Carr. Sys., 8: 237-269.
PubMed - Saad, W.A., L.I. Gutierrez, R.C. Vendramini, A.H.F. de Oliveira, L.A.A. Camargo and G. Garcia, 2005. Effect of pilocarpine and angiotensin II on salivary flow, total protein and electrolyte concentrations of saliva. Int. J. Pharmacol., 1: 190-194.
CrossRefDirect Link - Wong, C.F., K.H. Yuen and K.K. Peh, 1999. Formulation and evaluation of controlled release Eudragit buccal patches. Int. J. Pharm., 178: 11-22.
CrossRefPubMedDirect Link - Yamamoto, A., T. Iseki, M. Ochi-Sugiyama, N. Okada, T. Fujita and S. Muranishi, 2001. Absorption of water-soluble compounds with different molecular weights and calcitonin from various mucosal administration sites. J. Control. Release, 76: 363-374.
PubMed - Yang, T.Z., X.T. Wang, X.Y. Yan and Q. Zhang, 2002. Phospholipid deformable vesicles for buccal delivery of insulin. Chem. Pharm. Bull., 50: 749-753.
PubMed - Yousefzadeh, G., B. Larijani, B. Mohammadirad R. Heshmat, G. Dehghan, R. Rahimi and M. Abdollahi, 2006. Determination of oxidative stress status and concentration of TGF-β1 in the blood and saliva of osteoporotic subjects. Ann. N. Y. Acad. Sci., 1091: 142-150.
CrossRefDirect Link - Zakaria, Z.A., M.R. Sulaiman, A.M.M. Jais and M.N. Somchit, 2004. Effects of -amylase, protease and lipase on haruan (Channa striatus) mucus extract antinociceptive activity in mice. Pak. J. Biol. Sci., 7: 2202-2207.
CrossRefDirect Link - Zhang, J., S. Niu, C. Ebert and T.H. Stanley, 1994. An in vivo dog model for studying recovery kinetics of the buccal mucosa permeation barrier after exposure to permeation enhancers: Apparent evidence of effective enhancement without tissue damage. Int. J. Pharm., 101: 15-22.
CrossRef - Mohammadi, S.S. and M. Seyedi, 2008. Comparing oral gabapentin versus clonidine as premedication on early postoperative pain, nausea and vomiting after general anesthesia. Int. J. Pharmacol., 4: 153-156.
CrossRefDirect Link