
Luiz Fernando de Oliveira Varanda
Faculdade de Agronomia e Medicina Veterinaria, Universidade de Brasilia (UnB), ICC Sul, Campus Universitario Darcy Ribeiro, Cx. Postal 4508, Bras�lia, DF 70910-970, Brazil
Julia de Miranda Moraes
Faculdade de Agronomia e Medicina Veterinaria, Universidade de Brasilia (UnB), ICC Sul, Campus Universitario Darcy Ribeiro, Cx. Postal 4508, Bras�lia, DF 70910-970, Brazil
Ana Lourdes Arrais de Alencar Mota
Faculdade de Agronomia e Medicina Veterinaria, Universidade de Brasilia (UnB), ICC Sul, Campus Universitario Darcy Ribeiro, Cx. Postal 4508, Bras�lia, DF 70910-970, Brazil
Andre Rodrigues da Cunha Barreto-Vianna
Faculdade de Agronomia e Medicina Veterinaria, Universidade de Brasilia (UnB), ICC Sul, Campus Universitario Darcy Ribeiro, Cx. Postal 4508, Bras�lia, DF 70910-970, Brazil
Kaique Nogueira
Faculdade de Agronomia e Medicina Veterinaria, Universidade de Brasilia (UnB), ICC Sul, Campus Universitario Darcy Ribeiro, Cx. Postal 4508, Bras�lia, DF 70910-970, Brazil
Roberta Ferro de Godoy
Institute of Orthopaedics and Musculoskeletal Science, National Orthopaedics Hospital, University College of London, Brockley Hill Stanmore, HA7 4LP
Eduardo Mauricio Mendes de Lima
Faculdade de Agronomia e Medicina Veterinaria, Universidade de Brasilia (UnB), ICC Sul, Campus Universitario Darcy Ribeiro, Cx. Postal 4508, Bras�lia, DF 70910-970, Brazil
Asian Journal of Animal and Veterinary Advances
Year: 2016 | Volume: 11 | Issue: 3 | Page No.: 198-203







ABSTRACT
Slow speed and poor quality of bone healing are some of the major obstacles faced by equine veterinary practitioners. Cellular therapies that may assist in the osteogenesis process have been evaluated experimentally and clinically in several animal species and humans. The study evaluated the osteogenic effect of autologous percutaneous implantation of Mononuclear Cell Fraction (MCF) of the Bone Marrow (BM) on the healing process of experimentally induced fracture in the IV metacarpal bone by determining the Bone Mineral Density (BMD) in five horses of both sexes. Five days after experimentally inducing the bone fracture, the BM was aspirated from the sternum of each horse and the MCF was isolated. Subsequently, each horse was subjected to the percutaneous implantation of the MCF with DMEM in the right forelimb (treated limb-TL) and only DMEM as control, in the left forelimb (control limb-CL). The BMD values were higher in the TL compared to the CL in six of the eleven time intervals at which the bone density was measured. The results showed that MCF stimulated osteogenesis by accelerating the bone healing process and increasing the amount of mineralized bone matrix. The percutaneous implantation was found to be a minimally invasive low-cost technique that can replace sophisticated and labour intensive methods of stem cell transplantation.
PDF Abstract XML References Citation
How to cite this article
Luiz Fernando de Oliveira Varanda, Julia de Miranda Moraes, Ana Lourdes Arrais de Alencar Mota, Andre Rodrigues da Cunha Barreto-Vianna, Kaique Nogueira, Roberta Ferro de Godoy and Eduardo Mauricio Mendes de Lima, 2016. Osteogenic Effect of Percutaneous Implantation of Mononuclear Cell Fraction in Horses with Experimental Bone Fracture. Asian Journal of Animal and Veterinary Advances, 11: 198-203.
DOI: 10.3923/ajava.2016.198.203
URL: https://scialert.net/abstract/?doi=ajava.2016.198.203
DOI: 10.3923/ajava.2016.198.203
URL: https://scialert.net/abstract/?doi=ajava.2016.198.203
INTRODUCTION
The consolidation of a fracture consists of a complex repair mechanism which results in nearly complete restoration of normal bone architecture (Vo et al., 2012). In a biologically and mechanically favorable environment, Mesenchymal Stem Cells (MSCs) proliferate and differentiate into osteoblasts and chondroblasts (Guan et al., 2012). These cells produce an osteoid and cartilage matrix leading to formation of bone callus. The mineralized osteoid and cartilage matrix undergo endochondral ossification process until the fracture is completely filled by bony tissue. The MSCs are also precursor of the major cellular events involved in this process, such as chemotaxis, migration, proliferation and differentiation (Griffin et al., 2011). However, in the meantime the handling of this cell group has enabled new strategies for bone regeneration (Griffin et al., 2011).
In vivo studies have documented the osteogenic potential of MSCs in isolates of the Mononuclear Cell Fraction (MCF) as well as after the MSCs expansion in tissue culture. In addition, MSCs can maintain their viability and their potential to differentiate into various lineages after cryopreservation, increasing its viability for therapeutic use (Barberini et al., 2014). The BM contains osteoprogenitor cells that can be obtained by aspiration, thus making it either an effective bone graft by itself or a potentiating agent of the osteogenic action when combined with other materials such as cancellous or cortical bone grafts and demineralized bone matrix.
The technique of percutaneous injection of the MCF from the BM could be a relatively simple and cost effective method of induction of osteogenesis. The procedure is minimally invasive, avoids complications at the receptor site and can be repeated easily (De Oliveira Varanda et al., 2015). However, so far there are no studies reported regarding its use in horses. Thus, this study was aimed to evaluate the effectiveness of percutaneous implantation of MCF from bone marrow to repair experimentally induced surgical fracture of IV metacarpal bone in horses (IV MTC).
MATERIALS AND METHODS
Animals: Five horses of undefined breed, weighing an average of 248 kg and between 2.5 and 10 years of age that belonged to the Apprehension Section of the Secretariat of Agriculture, Livestock and Supply of the Federal District (SEAPA/DF, Brazil) were used. The animals underwent clinical examination, blood count and serum chemistry to determine their health status prior to the experiment. This study was approved by the Ethics Committee on Animal Use at the University of Brasilia (#48461/2010).
Surgically induced bone fracture: The food and water were withheld for 12 h prior to the surgical procedure to induce the experimental fractures. The horses were premedicated with 10% xylazine (1.0 mg kg–1, IV), the muscle relaxant, guaiacol glyceryl ether (110 mg kg–1, IV) and finally, anaesthesia was induced with ketamine hydrochloride (2.0 mg kg–1, IV). The animals were intubated with endotracheal tube and kept under inhalation anesthesia with isoflurane (15 mL kg–1), in semi-closed circuit. Antibiotic prophylaxis was done with potassium penicillin (20,000 IU kg–1, IV) before surgery.
With the animal placed in right lateral decubitus position, the left IV metacarpal bone (IV MTC) was accessed through a linear skin incision in the proximal third of the IV MTC bone and the 1 cm long bone fracture was created using a chisel and orthopedic hammer (Fig. 1) adopting an aseptic procedure. Subsequently, the incision was sutured, cleaned and a compressive bandage was placed at the fracture site. The animal was then placed in the left lateral decubitus and the procedure was repeated on the right limb.
During the post-operative period, the wounds were dressed daily and the horses were given systemic antibiotic therapy with benzathine penicillin (40.000 UI kg–1, IM) in three applications, every 48 h and analgesic anti-inflammatory phenylbutazone (4.4 mg kg–1, IV), once a day for five consecutive days.
 | |
| Fig. 1: | The 1 cm (bar) long bone fracture surgically induced in the IV MTC during the surgery (bar) |
 | |
| Fig. 2: | (a-b):(a) Needle positioned at the site of percutaneous implantation (arrow) at the time of the radiographic imaging to confirm the correct positioning and (b) Radiography in the dorsolateral-palmaromedial projection showing the correct location of the needle to perform the percutaneous implantation in the bone fracture |
Bone marrow collection and isolation of the mononuclear cell fraction: The BM was collected five days after creation of the bone fracture. The bone marrow sample was collected from the sternum. Immediately after collection, the mononuclear cell fraction was isolated in the laboratory, according to the protocol of De Oliveira Varanda et al. (2015). In the animal 1 (14.0×107 cells), animal 2 (10.2×107 cells), animal 3 (4.1×107 cells), animal 4 (4.4×107 cells) and animal 5 (3.5×107 cells) were collected.
Percutaneous implantation of MCF: A total of 5×107 nucleated cells in 1 mL of volume were standardized for the percutaneous graft. The animals were sedated with 10% xylazine (0.5 mg kg–1). Subsequently, hypodermic needle (21 gauge and 0.3 mm in length) was introduced at the site of bone fracture (Fig. 2a). The correct placement of the needle was confirmed by conventional radiography performed in the dorsolateral medial palmar-projection (Fig. 2b). The right forelimb (treated limb, TL) of each animal was injected with 1 mL of the MCF solution in DMEM and the left forelimb (control limb, CL) received 1 mL of DMEM only.
Radiographic analysis: Radiographic examinations to determine local bone regeneration were performed using a handheld conventional radiography equipment (Poskom PXP-40HF; Poskom Co., South Korea). The 45̊C oblique dorsolateral-palmar-medial projections were made on day 7 (D7-seven days after the percutaneous graft) and then weekly until day 56 and every 28 days until the day 140. The radiographs were evaluated for the BMD according to the degree of bone filling, on a six degrees varying scale.
The BMD was evaluated using an aluminum scale of 29 degrees with different thicknesses. The first degree was 1 mm, which increased 1 mm per degree until the last degree (Fig. 2a). The exposure factors were 62 kVp at 1.00 to 1.20 mAs, while the main beam was targeted between the IV metacarpal bone and the aluminum scale positioned parallel to each other, so that equal radiation amount and intensity were applied to both structures, with 70 cm standardized focus-film distance.
Images of IV metacarpal bone were analyzed using the Adobe Photoshop CS5 Extended software following the method proposed by Tavano et al. (2000). The "Histogram" tool allowed to measure the radiographic density of the area marked by the rectangle, on a grayscale (Fig. 3a, b).
Statistical analysis: The BMD results were evaluated statistically by means and standard deviation at 95% confidence level for each group at each evaluation time, using the student t-test.
RESULTS
The animals showed no lameness after recovery from anesthesia. The percutaneous implantation used to treat the bone fracture was found to be a minimally invasive procedure and easy to perform, which can be done without general anesthesia. No signs of infection or inflammatory reaction were observed after the implantation.
The degree of bone filling obtained from the radiographs of TL and CL at different times are presented in Table 1. Figure 4 shows the radiographs of TL and CL at different evaluation times.
No bone formation was observed in the area adjacent to the fracture region and adjacent soft tissue of any animal. The treated limbs had bone formation at the ends of the IV MTC and in the center of bone fracture, which was not observed in control limbs.
The BMD analysis showed significant differences between the mean BMD of treated and control limbs in six of the eleven times when the radiographs were performed.
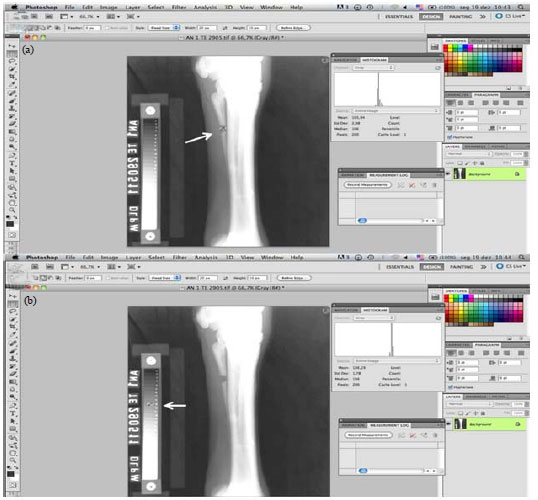 | |
| Fig. 3: | (a-b):Screen demonstration of the Adobe Photoshop CS5 software, which provides the radiographic density of the marked area (arrow) in (a) Gray levels and (b) The measurement of mineral density in scale (arrow) of 10 mm Al |
 | |
| Fig. 4: | Radiographic images of TL and CL at different evaluation times |
The BMD values of the groups are shown in Table 2.
DISCUSSION
The MCF implantation was performed five days after the bone fracture following the methodology of De Barros et al. (2001). The differences between the TL and CL was observed at 6 of the 11 evaluation times. Corroborating the results of De Barros et al. (2001), the formation of bone tissue was observed in the TL as determined by the radiopacity in the center of the bone fracture, which did not occur in CL. It was also observed that the animal in which different bone filling was detected between the TL and the CL only in four evaluation times had lower cellularity. It was deduced that the MSCs present in the MCF of the BM might have differentiated into bone tissue and that the quantity of mononuclear cells of BM and MSCs implanted directly influenced the speed of bone repair process in horses.
Some authors have reported that the amount of MSCs (Guan et al., 2012) and growth factors (Gao et al., 2012) in the
| Table 1: | Degrees of bone regeneration obtained by analyzing the TL and CL at different evaluation times |
 | |
| The degree values were obtained using the mode of degrees evaluated by five evaluators, *Times where the TL was graded higher than the CL | |
| Table 2: | Mean and standard deviation values of Bone Mineral Density (BMD) in millimeters of aluminum (mm Al) in the Treated Limb (TL) and Control Limb (CL) at different evaluation times |
 | |
| Times where there was a significant statistical difference between TL and CL according to student’s t-test | |
BM decrease with age and the osteogenic potential of the MCF therapy in older animals could be reduced. However, this fact was not conspicuous in the present study (Table 1).
The results supported the concept that osteogenesis could be stimulated by BM MCF implanted percutaneously and this stimulation is related to the presence of osteoprogenitor cells as it has been described by De Barros et al. (2001). Furthermore, the application of BM MCF effectively resulted in early bone filling compared to the control.
The BM MCF has osteogenic capacity, which could be favored by the presence of growth factors, released during the inflammatory process on the 5th postoperative day. The existence of these factors may be important in the repair as observed by Vo et al. (2012).
CONCLUSION
In addition to the therapeutic action of MSCs, early bone formation may have been influenced by growth factors released by degranulation of platelets present in the MCF. Thus, this procedure can also be used in chronic situations to either start or restart the repair process as in the case of delayed union, nonunion, congenital malformation and resection of neoplasia.
The percutaneous implantation of MCF was minimally invasive, inexpensive and can be performed without general anesthesia. The technique is feasible owing to its fast processing and the possibility of performing it soon after the injury.
REFERENCES
- Barberini, D.J., N.P.P. Freitas, M.S. Magnoni, L. Maia and A.J. Listoni et al., 2014. Equine mesenchymal stem cells from bone marrow, adipose tissue and umbilical cord: Immunophenotypic characterization and differentiation potential. Stem Cell Res. Ther., Vol. 5.
CrossRefDirect Link - Griffin, M., S.A. Iqbal and A. Bayat, 2011. Exploring the application of mesenchymal stem cells in bone repair and regeneration. J. Bone Joint Surg. Br., 93: 427-434.
CrossRefDirect Link - De Barros, S.V.D.S.G., R.J. Del Carlo, M.I. Viloria, S.R. Galvao, A.M. Filho and D.R. Oliveira, 2001. [Percutaneous bone marrow autograft. II. Repair of segmentar defects produced in the radii rabbit] Cienc Rural, 31: 627-632, (In Portuguese).
CrossRefDirect Link - Gao, C., J. Seuntjens, G.N. Kaufman, N. Tran-Khanh and A. Butler et al., 2012. Mesenchymal stem cell transplantation to promote bone healing. J. Orthop. Res., 30: 1183-1189.
CrossRefPubMedDirect Link - Guan, M., W. Yao, R. Liu, K.S. Lam and J. Nolta et al., 2012. Directing mesenchymal stem cells to bone to augment bone formation and increase bone mass. Nat. Med., 18: 456-462.
CrossRefDirect Link - De Oliveira Varanda, L.F., J. de Miranda Moraes, J.V.F. Sales, A.L.A. de Alencar Mota, A.R. da Cunha Barreto-Vianna, R.F. de Godoy and E.M.M. de Lima, 2015. Collection and isolation of mesenchymal stem cells from equine bone marrow. Online J. Vet. Res., 19: 216-223.
Direct Link - Vo, T.N., F.K. Kasper and A.G. Mikos, 2012. Strategies for controlled delivery of growth factors and cells for bone regeneration. Adv. Drug. Delivery Rev., 64: 1292-1309.
CrossRefDirect Link