
Mohammed A. Alsaif
Department of Community Health Sciences College of Applied Medical Sciences
P.O. Box 59854, King Saud University Riyadh-11535, Saudi Arabia
Journal of Medical Sciences
Year: 2004 | Volume: 4 | Issue: 4 | Page No.: 287-293







ABSTRACT
Anti-ulcerogenic potential of boric acid (BA) was investigated using five models of gastric lesion induced in experimental Wistar rats: (1) HCl/ethanol-induced gastric lesions, (2) Absolute ethanol-induced gastric lesions, (3) Indomethacin-HCl/ethanol-induced gastric lesions, (4) Pylorus ligation-induced gastric lesions and (5) Hypothermic restraint stress-induced gastric lesions. In all the models studied, the antiulcer activity of BA was compared with that of cimetidine (100 mg kg-1 p.o.). In models 1, 2, 3 and 5: ulcer index and mucus production was determined. In pylorus ligated rats ulcer index, mucus production, total volume of gastric juice and gastric acidity level were measured. Administration of BA to the rats by oral route (60-240 mg kg-1) dose-dependently prevented the formation of acute gastric lesions in all five models of ulceration. The dose-dependent reduction of lesion formation was in all cases accompanied by significant increases in gastric mucus production. In pylorus ligated rats, total volume of gastric juice and gastric acidity was significantly decreased as compared to control group, these result similar to that produced by cimetidine. The cytoprotective effect of BA against HCl/ethanol induced ulceration was significantly reversed by prior treatment with a dose (20 mg kg-1 ip) of indomethacin that inhibits prostaglandin biosynthesis. The results of this study demonstrate that BA has both prophylactic and curative effects on various experimentally induced gastric ulcers.
PDF Abstract XML References
How to cite this article
Mohammed A. Alsaif, 2004. Gastric Antisecretory and Antiulcer Activity of Boric Acid in Rats. Journal of Medical Sciences, 4: 287-293.
DOI: 10.3923/jms.2004.287.293
URL: https://scialert.net/abstract/?doi=jms.2004.287.293
DOI: 10.3923/jms.2004.287.293
URL: https://scialert.net/abstract/?doi=jms.2004.287.293
INTRODUCTION
Boric acid (boracic acid, orthoboric acid) is an inorganic acid form with the chemical formula H3BO3. Compounds of boron have been used for a variety of applications: food preservatives, water softeners, pH adjusters, emulsifiers, neutralizers, stabilizers, buffers and viscosifiers[1] and also recognized as an essential plant micronutrient for growth[2] and there is growing evidence of its essentiality in animals and human beings[3-5]. The major source of boron to human beings is diet (e.g. fruits, vegetables, nuts) and water[6].
Boric acid is rapidly absorbed after its administration, is distribute through the body water via passive diffusion, is not metabolized and is excreted from the body via urine[7]. The half-life time (t½) of BA is approximately in the order of one day and it does not appear to accumulate in soft tissue, but in bones[8] Blech et al.[9] demonstrated that a 3% BA solution helped to improve dramatically the healing of deep wounds. Patients who were treated with BA returned to a normal care unit about three times more rapidly (mean 20 days) than those who received conventional antiseptics, such as chlorhexidine or iodinated polyvinylpyrolidone (mean 55 days)[10].
Boric acid has been widely used in the management of open wound and trophic ulcers[11]. In view of its vast medical utilization and other uses of boron compounds as pH adjusters and neutralizers the present study was designed to investigate BA for its affects on the gastric mucosa subjected to HCl/ethanol solution, absolute ethanol, indomethacin, pylorus ligation and hypothermic stress.
MATERIALS AND METHODS
Animals: Male Wistar albino rats (bred at the Experimental Animal Care Center, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia) of roughly the same age, weighing 180-220 g, were used for the present study. All the animals were maintained under controlled condition of temperature, humidity and light and were provided with Purina chow and water ad libitum. The rats were randomly assigned to control and treatment groups (6 rats in each group) and were fasted for 48 h with free access to drinking water.
HCl/ethanol-induced gastric mucosal membrane lesions: An aqueous solution of BA or distilled water alone was administered by gavage to the test rats 30 min before oral administration by gavage of 1mL HCl/ethanol solution (150 mM HCl in 60% v/v ethanol). The rats were sacrificed 1 h later using ether and the stomachs were removed and observed for lesions in the glandular portion. The ulcers were scored according to the method of Valcavi et al.[12]. The deep linear ulcers more than 100 mm in length = 6 and less than 100 mm in length = 3 were counted. The scores of each single lesion were then summed up for the determination of ulcer index.
Absolute ethanol-induced gastric membrane lesions: Absolute ethanol-induced lesions were produced using the method described above for the HCl/ethanol-induced lesion. The rats received the test drug on vehicle followed 1 h later by 1 mL of absolute ethanol by oral route. They were also killed after 1 h of ethanol administration using ether and the lesions formed were observed and scored.
HCl/ethanol-induced lesions in rats pre-treated with indomethacin: The effect of pre-treatment with indomethacin on the preventive effect of BA on HCl/ethanol-induced gastric lesions was studied following a modification of the method described by Sun et al.[13]. All the rats received indomethacin (20 mg kg-1) by intraperitoneal route. One hour later, the test rats received BA or cimetidine while the controls received 1 mL of vehicle by oral route. This was followed after an hour later by oral administration of 1 mL of the HCl/ethanol solution. The rats were then sacrificed 1 h later using ether and the stomachs were observed for lesions.
Pylorus-ligated gastric secretion and ulceration: Following a 48 h fasting, the test drugs and vehicle were administered orally to the test and control rats, respectively, 1 h before the experiment. The pylorus of each rat was tied under light ether anesthesia and the abdominal incisions were closed. The rats were sacrificed 6 h later and the gastric juice produced by each rat was collected separately in a centrifuge tube[14]. The gastric contents was measured, centrifuged and subjected to analysis for titratable acidity against 0.01 N NaOH to pH 7 using a pH meter and the total acid output was calculated. Ulcers formed in the glandular portion of the stomachs were scored as previously described[12].
Hypothermic restraint stress-induced gastric ulcers and mucus contents: The method of Levine[15] was followed with slight modification. The animals were fasted for 48 h with access to water ad libitum. One hour after receiving the drug treatment, the rats were immobilized in restraint cages and placed inside a ventilated refrigerator maintained at a temperature of 2-4°C for 2 h. After exposure to restraint-hypothermic stress animals were sacrificed and stomachs were examined for the severity of intraluminal bleeding according to the following arbitrary scale: 0, no blood detectable; 1, thin blood follows the rugae; 2, thick blood follows the rugae with blood clots in certain areas; and 3, extensive covering of the whole gastric mucosal surface with thick blood[16]. After wiping the blood off the lesions, each stomach was scored according to the method of Valcavi et al.[12].
Measurement of mucus production: Gastric mucus production was measured in the rats that were subjected to HCl/ethanol-, absolute ethanol-and indomethacin/HCl-ethanol-induced lesions. After estimating the degree of lesion formation, the gastric mucosa of each rat was gently scraped using a glass slide and the mucus obtained was weighed using a precision electronic balance.
Histopathological procedures: Tissue samples were preserved in 10% buffered formalin and processed for routine paraffin block preparation. Using an American Optical Rotary Microtone, sections of thickness about 5 μm were cut and stained with haematoxylin and eosin. These were examined under the microscope for histopathological changes such as congestion, corrosion, hemorrhage and necrosis by an observer who was blind with respect to the treatment groups. The severity of histopathological changes was expressed according to an arbitary scale[17].
Statistical analysis: Values in tables are given as arithmetic means±standard error of the mean (SEM). The significance of differences between means was calculated using the Student’s t-test.
RESULTS
HCl/ethanol induced gastric lesions: The characteristic striated lesions, which result from the oral intake of the HCl/ethanol solution, were found in the glandular portion of the rat stomachs. BA pretreatment provided a significant dose dependent protection against ulceration caused by HCl/ethanol. The mean ulcer index was reduced from the 19.83 control value to 9.83 for the group which received 120 mg kg-1 of the BA. At the dose of 240 mg kg-1 BA, the ulcer intensity reduced 92% as compared to control group. Mucus production also increased dose-dependently from 35 to 44 mg as the dose of BA increased from 60 to 240 mg kg-1 compared with 27 mg for the controls. Although cimetidine (100 mg kg-1) had a less significant inhibition of lesion formation [48% compared with BA (240 mg kg-1)], however, it significantly reduced the ulcer index and increased mucus production as compared to controls rats (Table 1).
Indomethacin/(HCl/ethanol)-induced gastric lesions: Table 2 shows the effect of giving indomethacin to the rats 1 h before the BA on the protective effect of the BA against HCl/ethanol solution. Indomethacin significantly reduced the protective effect produced by BA at the dose of 240 mg kg-1. Thus the prevention of lesion formation reduced from 92% for the highest dose of BA (Table 1) to 36% after indomethacin pretreatment (Table 2). This was accompanied by a similar reduction in mucus production both for the control group and all the BA treated groups. Lesion inhibition and mucus production were also reduced significantly for cimetidine.
Absolute ethanol-induced gastric lesions: Table 3 shows the results obtained when absolute ethanol was used as the necrotizing agent. The gastric lesions obtained were morphologically similar to those obtained using the HCl/ethanol solution. BA produced dose-dependent inhibition of lesion formation but the effect was not as marked as compared with the effect obtained with HCl/ethanol solution (Table 1). The level of inhibition was 49% for the dose of 240 mg kg-1 representing a drop of 43%. Mucus production was increased dose-dependently from 12% at the lower dose (60 mg kg-1) to 58% at the higher dose (240 mg kg-1) of BA treatment. Pretreatment with cimetidine (100 mg kg-1) produced, significant reduction in ulcer index and a significant increase in mucus production as compared to control.
Pylorus ligation-induced lesions and gastric acid secretion: Pylorus ligation for 6 h resulted in the accumulation of gastric secretion and increase in the titratable acidity. BA produced dose-dependent significant decrease in the volume of gastric juice, titratable acidity and ulcer index as compared to control (Table 4). Similar effects were seen with cimetidine treatment. However, these effects were accompanied by significant dose-dependent increase in mucus production as compared to control Shay rats.
Hypothermic restraint stress-induced lesions: The animals subjected to restraint plus cold for 2 h showed the presence of considerable ulcerogenecity in the form of hemorrhagic mucosal lesions in the stomach. The area of involvement in all the animals was confined to the glandular segment only. There was also evidence of intraluminal bleeding in these animals. Treatment with BA produced a significant and dose dependent decrease in the gastric lesions. BA also produced significant dose-dependent decrease in intraluminal bleeding. Cimetidine (100 mg kg-1) treatment also significantly reduced the intraluminal bleeding but it failed to produce any reduction in the ulcer index (Table 5).
| Table 1: | Effect of boric acid on gastric lesions induced by HCl/ethanol in rats |
 | |
| Table 2: | Effect of pre-treatment with indomethacin on the protective effect of boric acid against gastric lesions induced by HCl/ethanol |
 | |
| Table 3: | Effect of boric acid on gastric lesions induced by absolute ethanol in rats |
 | |
| Table 4: | Effect of the boric acid on pylorus ligation-induced gastric secretion in the rats |
 | |
| Table 5: | Effect of boric acid on hypothermic restraint stress induced gastric ulcers in rats |
 | |
| *p<0.05, **p<0.01 and ***p<0.001 Student’s t-test, All treated groups were statistically compared to control group, Six rats were used in each group | |
| Table 6: | Effect of boric acid on the induction of gastric mucosa histopathological lesions by treatment with 1 mL of HCl/ethanol (150 mM HCl in 60% v/v ethanol) |
 | |
| - = normal + = little effect ++ = appreciable effect +++ = severe effect | |
Effects on histopathological gastric lesions: HCl/ethanol treatment caused considerable damage in the form of necrosis, corrosion, congestion and haemorrhagic mucosal lesions in the stomach walls of treated animals.
However, no neutrophilic component was evident. The area involved was mainly the glandular segments. There was also evidence of interluminal bleeding in these animals. Pretreatment with BA provided significant and dose-dependent protection against the action of HCl/ethanol (Fig. 1-4).
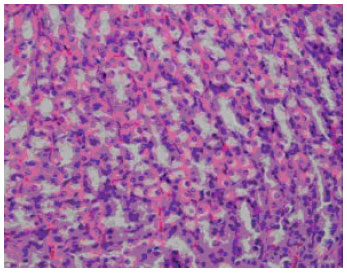 | |
| Fig. 1: | The stomach wall of a control rat showing its normal appearance. Haemotoxylin and eosin, x 40 |
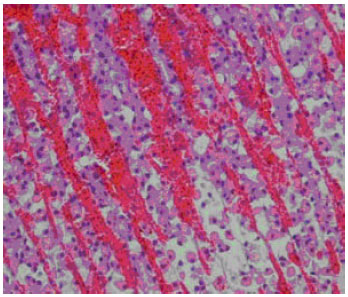 | |
| Fig. 2: | The stomach wall of a rat after treatment with 1 mL HCl/ethanol, by gavage. Haemotoxylin and eosin, x 40 |
The histopathological results showed that, the higher dose (240 mg kg-1) of BA produced complete protection against the damage (Table 6).
DISCUSSION
The results of the present study clearly suggest that BA offers dose-dependent protection against the ulceration caused by absolute ethanol, HCl/ethanol, indomethacin/HCl/ethanol and hypothermic restraint stress. The histopathological studies revealed that pretreatment with BA inhibited the HCl/ethanol-induced congestion, haemorrhage, corrosion and necrosis in gastric mucosa (Fig. 3 and 4).
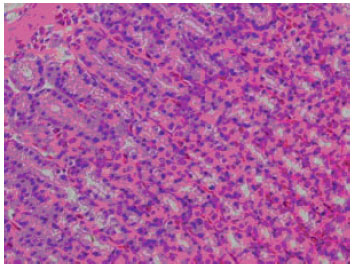 | |
| Fig. 3: | The stomach wall of a rat after treatment with boric acid (120 mg kg-1) and 1 mL HCl/ethanol by gavage. Haemotoxylin and eosin, x 40 |
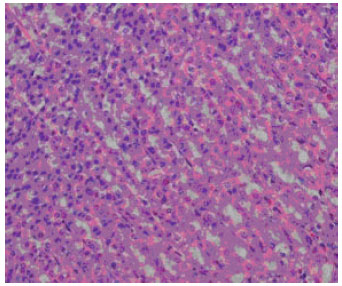 | |
| Fig. 4: | The stomach wall of a rat after treatment with boric acid (240 mg kg-1) and 1 mL HCl/ethanol by gavage. Haemotoxylin and eosin, x 40 |
It also produced a dose-dependent decrease in basal and HCl/ethanol stimulated gastric acid secretions in rats. The increase in gastric acid output is considered to contributes to the development of peptic ulceration and is often termed as ‘aggressive’ factor[18].
The results show that the BA is capable of nearly completely (92%) inhibiting the lesion formation by HCl/ethanol at the dose of 240 mg kg-1. Although the effect reduced significantly when absolute ethanol was used as the necrotizing agent, the dose-dependent response was evident in all the experiments. The accompanying significant dose-dependent increases in mucus production as the dose of BA was increased suggests that the gastric mucosal strengthening mechanism contributes to the anti-irritant potential of BA. It is evident from the pylorus ligation experiment that the protection offered by BA against the HCl/ethanol solution is not due to an acid-neutralizing effect. The dose-dependent ability of BA to prevent lesions of absolute ethanol origin also supports this view. The pathogenesis of ethanol-induced gastric mucosal damage in rats is complicated because of the release of tissue-derived mediators such as histamine and leucotriene C4. These mediators act on gastric microvasculature, triggering a series of events that lead to mucosal and possibly submucosal tissue damage[19]. The cytoprotective action of BA may therefore include mechanisms other than simple acid neutralization.
The ability of BA to produce significant inhibition of indomethacin induced ulcers suggests its potential antiulcer activity. Suppression of mucosal generation of PGs by indomethacin and other nonsteroidal anti-inflammatory drugs (NSAIDs) cause mucosal damage and increase the risk of the formation or exacerbation of peptic ulcer[20]. The compounds with the ability to generate PGs in gastrointestinal tract have been shown to protect gastric mucosa against various ulcerogenic agents[21]. Peskar[22], reported that the gastric mucosal lesions induced by NSAIDs are accompanied by increase in the leukotrien production.
Our results revealed that BA significantly protected gastric mucosa against hypothermic restraint stress induced lesions and mucus depletion. The ability of cold restraint stress to decrease gastric wall mucus has been demonstrated previously[23]. The gastric mucus coat is thought to be important for preventing damage and for facilitating repair of the gastric epithelium[24]. However, there is considerable controversy regarding the role of mucus in prevention of gastric mucosal injury[25]. Bottcher et al.[26], reported that N-acetyl-cysteine protected gastric mucosa against necrotizing agents while reducing gel mucus thickness, suggesting that gastric mucus is not of primary importance as one of the mechanisms whereby protective agents mediate the preservation of gastric mucosa against ulcerogenic agents.
In conclusion, this study demonstrate that BA possesses significant antiulcer and cytoprotective effects on various experimentally induced gastric lesions. Further studies are necessary to elucidate its exact mode of action and therapeutic value in the prophylactic and/or treatment of gastric ulcer.
REFERENCES
- Woods, W.G., 1994. An introduction to boron: History, sources, uses and chemistry. Environ. Health Perspect., 102: 5-11.
PubMed - Moseman, R.F., 1994. Chemical disposition of boron in animals and humans. Environ. Health Persoect., 102: 113-117.
PubMed - Shay, H., S.A. Komarow, S.S. Fels, D. Meranze, M. Gruenstein and H. Siplet, 1945. A simple method for the uniform production of gastric ulceration in the rat. Gastroenterology, 5: 43-61.
Direct Link - Al-Bekairi, A.M., S. Qureshi, M.M. Ahmed, M. Afzal and A.H. Shah, 1992. A study of uric acid pretreatment for the protection of rat gastric mucosa against toxic damage. Food Chem. Toxicol., 30: 525-531.
PubMed - Oates, P.J. and J.P. Hakkinen, 1988. Studies on the mechanism of ethanol-induced gastric damage in rats. Gastroenterology, 94: 10-21.
PubMedDirect Link - Franzone, J.S., R. Cirillo and C. Cravenzola, 1988. Cytoprotective activity of deboxamet: A possible interference with prostaglandin and prostacyclin metabolism in rat gastric mucosa. Int. J. Tissue React., 10: 149-158.
PubMed - Peskar, B.M., U. Hoppe, K. Lange and B.A. Peskar, 1988. Effect of non-steroidal anti-inflammatory drugs on rat gastric mucosal leukotriene C4 and prostanoid release: relation to ethanol-induced injury. Br. J. Pharmacol., 93: 937-943.
Direct Link - Ruzick, T., T. Simmet, B.A. Peskar and O. Braun-Falco, 1984. Leukotrienes in skin of atopic dermatitis. Lancent, 323: 222-223.
CrossRef - Robert, A., W. Bottcer, E. Golanska and G.L. Kauffman, Jr., 1984. Lack of correlation between mucus gel thickness and gastric cytoprotection in rats. Gastroentrology, 86: 670-674.
PubMed